Individual features of the child. Kataeva A., Strebeleva E.A. Preschool oligophrenopedagogy: Studies. for stud. higher studies, institutions

 Live journal
Live journal Facebook
Facebook Twitter
Twittern1.doc
CHAPTER 2. AGE FEATURES OF CHILD DEVELOPMENT.
Features of psychomotor development of children of the 1st year of life
A feature of children of the 1st year of life is a large developmental dependence on the impact of an adult. Communication with adults is a necessary need of children in the first months of life, the source of their development.The rapid pace and unevenness of development determine the division of the 1st year of life into qualitatively different periods, highlighting in each period skills that are essential for the further development of the child. These skills are called leading, and it is on them that the educational influence of adults should be directed.
In the period newborn it is still difficult to single out the leading one, but there are basic tasks of upbringing: careful hygienic care, ensuring the well-being and calm of the child; the formation of a clear rhythm of feeding, the formation of positive and the prevention of negative habits (sucking fingers, nipples, motion sickness, indiscriminate feeding, etc.). By the end 1st month the daily rhythm is formed with the concentration of sleep at night, and wakefulness during the day. During wakefulness, it is necessary to maintain a calm and active state of the child, to cause tracking and listening, to spread the child on his stomach, prompting him to raise his head.
Since the end of the neonatal period up to 3 months the duration of wakefulness is increased, a clear alternation of sleep and wakefulness is formed during the day, a positive attitude towards feeding, sleeping and hygienic procedures is fostered. Leading the development of the child is the formation of visual and auditory orienting reactions, as well as the response of emotional and positive reactions. The ability to focus on the hanging toy, the face of an adult, to follow a moving object develops. The child listens to the sounds (speech, singing, rattles sound), develops "speech hearing", the ability to establish a connection between visual and auditory impressions, perceive the environment at a distance using distant analyzers. In the end 1st - the beginning of the 2nd month there is a response smile to the communication of an adult. On 3rd month a complex of revival is formed: while rejoicing, the child straightens his arms, unclenches his fingers, encounters a toy, makes sounds (gurgles, glitters). There are observed the retention of the head in a horizontal and vertical position and the support of the legs.
At the age of 4 - 6 months the duration of wakefulness continues to increase, a positive attitude towards processes is being formed, and activity during feeding is developing.
Leading in this age period are the further development of visual and auditory orienting reactions, orientation in the environment, on the basis of which speech understanding, activity, sensory perception and complex behavior are formed later. On 4th month tracking, auditory and visual concentration in any position are improved (lying on the back, on the stomach, on the hands of an adult). Visual, auditory, motor, and tactile interconnections are established: the child finds the source of the sound with his eyes (localizes the sound in space), for a long time examines the object that has attracted the attention, the picture, the bright spot, of the other child. This is the basis of the formation of the ability to observe and communicate with each other children.
AT 4 - 5 months the child is able to distinguish the intonation of the speech addressed to him, the melody (dance, calm), the voice of familiar and unfamiliar adults, to recognize the mother or another close person. TO 5 monthsthe child reacts to a new environment; in unfamiliar conditions, at the sight of strangers, ceases to smile, examines them for a long time and intensely, and may cry. If they speak strictly to him, he frowns, squeezes his lips, shows discontent. AT 6 months the child knows his name by sound.
Leading in age 4 - 6 months is the development of hand movements: its main functions - the ability to take, hold, manipulate, to 5 months - the act of grabbing, purposeful movement of the hands, at 6 months the child himself takes the toys and manipulates them. Based on these movements, game actions with objects are formed; the child learns the environment, gains life experience. Hand movements in many ways contribute to the formation of skills in the process of feeding and basic movements in the second half of the year.
Leading is the development of the preparatory stages of active speech. At this age, the boom develops rapidly and the background of babbling appears. In 4 months the child is walking for a long time, by 5 months it turns into a melodious gait, colored by different intonation. To 5 - 6 months the child begins to pronounce consonant sounds (labial, palatine - n, b, t, d, n, l and others) and the first syllables are a combination of a vowel and a labial or palatal consonant sound ( na, ba, ma and others), i.e. babbling appears. At the same time, the role of the articulatory apparatus and auditory concentration, "speech hearing" is great. The child hears the sounds uttered by the adult, listens to himself and begins to pronounce the sounds and syllables again, which contributes to the pronunciation of the first words in the second half of the year of life.
TO 6 months the child lies on his stomach, leaning on the palms of straightened hands, turns over from his back to his stomach and back, crawls up, firmly rests his legs with the support under his arms. By the end of the first half of the year, the child may be awake independently, actively and for a long time.
At the age of 7 - 9 months the duration of wakefulness is increased to 2–2.5 hours; the child switches to a regimen with three periods of daytime sleep. As development progresses, its behavior in regime processes becomes more complex. He drinks from a cup held by an adult, and by 9 months holding her hands, holds in his hand a crust of bread.
Leading at this age is the development of movements, and above all the mastery of crawling. TO 7 months baby creeps well. This changes his behavior, he becomes more active and independent, begins to navigate the environment. Crawling has a positive effect on physical development; in a crawling child, the muscles of the legs, arms, back, abdominals, neck, strengthen, the correct posture is formed.
TO 8 months there is a jump in the development of movements - the child acquires a vertical position, knows how to sit, lie down, stand up, sit, stand, cross, walk, hold, along the barrier.
During the period 7 - 9 months he begins to understand the speech of an adult. It changes his behavior, the nature of activities, movements, affects the active speech. TO 7 months the child, at the request of the adult, finds with a glance an object that is in a permanent place, repeatedly shown and called to it. TO 8 months he finds a few items by the word of an adult, starts performing simple actions (without showing) - "ladies", "goodbye" at the request. TO 9 months he understands the names of several objects, finds them anywhere, using the pointing gesture, knows his name, gives the toy in his hands. The child understands the words associated with the regime processes, performs at the request of the adult movement and action ("sit down", "drink", "give a pen"). The adult's speech begins to regulate the actions of the child.
At this age, the ability to imitate babble and actions with objects develops. Without the ability to imitate the further development and training of the child is impossible.
TO 7 months children re-pronounce individual syllables - babble. Each child has “his” two or three syllables, which he repeatedly, repeatedly, pronounces in various combinations. By 8 months, he repeats these syllables for adults, and in 9 - 10 months easily repeats after adults new syllables that have not yet pronounced. It enriches babble. The child accompanies his movements, actions, communication with adults and children with babbling.
WITH 7 months actions with objects, repeated, identical with all, to 8 months - different depending on the properties of the toy, to 9 monthsimitating the adult, the child masters new actions, reproduces the learned dance movements to a certain melody.
At the age of 10 - 12 months the child is active in the process and begins to show independence in feeding. Develop the movement. He still crawls, but often gets up, walks a lot, climbs a hill, etc., to 12 months walks without holding, for a long time and in different directions.
A child acquires a lot of new things with the development of speech understanding. TO 10 months he, at the request of an adult, finds and brings a familiar toy, if it is in his field of vision, to 11 months finds a toy called among many others, and to 12 months at the request of an adult, he finds several homogeneous objects if they outwardly differ slightly (different dolls, balls of different sizes and colors, etc.). By the end of the year, some words in the speech of an adult begin to acquire a generalized character for the child. The child understands the word "no" if it is pronounced according to the situation. It becomes possible to influence through speech on his behavior. The number of understood words denoting the names of toys, clothes, furniture, actions, movements, the names of adults and children, body parts, etc. is increasing. It can perform simple tasks, respond adequately to the words "can", "good", "bad".
During the period 10 - 12 months active speech is formed, the child masters the first words. At the heart of pronouncing the first words is the understanding of speech, the ability to babble and imitate. By the year the child speaks about 10 simple, lightweight, "babbled" words with which he begins to denote certain concepts. The number of spoken words is much less understood. A baby babbles a lot, babble accomplishes its actions and movements. Individual words and sounds, supported by facial expressions, begin to serve as a means of communication with adults and children.
Under the influence of understanding the speech complicate the actions with objects. AT 10 - 12 months child learns to perform actions on the show and the word of an adult. They become more diverse and focused. Hand movements are coordinated. He performs actions aimed at achieving the result: close, open, insert, remove, remove, put on. He imposes a brick on a brick, removes and puts on rings, rolls balls along the chute and - others. The number of actions performed with one object increases, the child learns to transfer actions mastered with one object to another. The number of toys used by the child is increasing. His actions become sustainable: he strives to achieve the goal, enjoys the result obtained. There is an imitation of an adult in actions with story toys. At the request of an adult, he, at the sight of a toy, reproduces what the adult had taught him: he rolls the car, feeds the doll, craps, etc. There are prerequisites for the game. This is a period of development of objective activity based on imitation and reproduction of the learned.
Features of the development of young children (1-3 years)
Age from 1 year to 3 years is a period of significant changes in the life of a small child. First of all, the child begins to walk. Having the opportunity to move independently, he masters the far space, independently comes into contact with a mass of objects, many of which had previously remained inaccessible to him.As a result of this "release" of the child, decrease. his dependence on an adult is rapidly developing cognitive activity, objective actions. At the 2nd year of a child’s life, the development of objective actions is observed, and at the 3rd year of life, the objective activity becomes leading. By the age of three, his leading hand is determined and the coordination of the actions of both hands begins to take shape.
With the emergence of objective activity, based on the assimilation of precisely those methods of action with an object that ensure its use for its intended purpose, the child’s attitude to the surrounding objects changes, the type of orientation in the objective world changes. Instead of asking, "What is this?" When a child encounters a new object, the question “What can be done with this?” arises. However, this interest is extremely expanding. Thus, with a free choice of objects and toys, he seeks to get acquainted with as many of them as possible, involving objects in his activities.
In close connection with the development of objective actions, the child’s perception develops, since in the course of actions he acquaints himself not only with the methods of their use, but also with their properties - form, size, color, mass, material, etc.
Children have simple forms of visual-effective thinking, the most primary generalizations directly related to the release of certain external and internal signs of objects.
At the beginning of early childhood, the child’s perception is still extremely poorly developed, although in everyday life he seems to be quite oriented. Orientation occurs, rather, on the basis of the recognition of objects, than on the basis of genuine perception. Recognition itself is associated with the selection of random, conspicuous signs - landmarks.
The transition to a more complete and comprehensive perception occurs in the child in connection with the mastering of objective activity, especially instrumental and correlative actions, during which he is forced to focus on different properties of objects (size, shape, color), bringing them in line with a given attribute. First, the correlation of objects and their properties occurs practically. This practical correlation then leads to perceptual correlations. The development of perceptual actions begins.
The formation of perceptual actions in relation to different content and different conditions in which this content is embodied, occurs non-simultaneously. In relation to more difficult tasks, a young child can remain at the level of chaotic actions, without taking into account the properties of the objects with which he acts, at the level of actions with the use of force that do not lead him to a positive result; in relation to tasks that are more accessible in content and closer to the child’s experience, he can proceed to practical orientation - to samples, which in some cases can provide a positive result of his activity; in a number of tasks, the child moves on to perceptual orientation itself.
Although a child at this age rarely uses visual correlation, but uses extensive “try-on,” however, it provides a better account of the properties and relationships of objects, provides more opportunities for a positive solution of the problem. Mastering "primerivanie" and visual correlation allows young children not only to produce differentiation of the properties of objects at the "signal" level, i.e. to search, detect, distinguish and identify objects, but also to display the properties of objects, their true perception based on the image. This is reflected in the ability to make a choice on the model. The close connection between the development of perception and activity is manifested in the fact that the choice according to the model first begins to be made by the child in relation to form and size, i.e. in relation to the properties that must be considered in practical action, and only then in relation to color (LA Wenger, VS Mukhina).
The development of speech in this period is particularly intense. Mastering speech is one of the main achievements of the child of the 2nd - 3rd years of life. If by the age of 1 year the child almost does not speak at all, having 10 to 20 babbled words in the dictionary, then by three years his dictionary has more than 400 words. Throughout the early years, speech is becoming increasingly important for the entire mental development of the child. It becomes the most important means of transmitting public experience to a child. Naturally, adults, directing the perception of the child, actively use the names of the properties of objects.
The emergence of speech is closely related to the activities of communication. It appears for communication purposes and develops in its context.
The need for communication is formed with the active influence of an adult on a child. A change in the forms of communication also occurs with the initiative influence of an adult on a child. Thus, in early childhood, we can note the rapid development of the following mental areas: communication, speech, cognitive (perception, thinking), motor and emotional-volitional.
Mental assessment parameters
Diagnosis of the mental development of children shows the real achievements of the child, established in the course of education and training. It should be borne in mind that in cases of serious problems in mental development, it is necessary to apply not only the method of psychological and pedagogical experiment, but also other methods: study of the child’s developmental history; monitoring the behavior of the child, his game; in more difficult cases - clinical, neurophysiological, pathopsychological, etc.The main parameters for assessing the cognitive activity of young children can be considered: acceptance of the task; ways to complete the task; learnability in the survey process; attitude to the result of its activities.
Acceptance of the task, i.e. The consent of the child to perform the proposed task, regardless of the quality of the execution itself, is the first, absolutely necessary condition for the execution of the task. In this case, the child shows interest either in toys or in communication with adults.
Ways to complete the task: self; with the help of an adult, i.e. diagnostic training is possible; self after training.
Adequacy of actions is defined as the compliance of the child’s actions with the conditions of this assignment, dictated by the nature of the material and the requirements of the instruction. The most primitive way is the action of force or chaotic action without taking into account the properties of objects.
Inadequate performance of the task in all cases indicates a significant impairment of the child’s mental development.
Learning is carried out only within the tasks that are recommended for children of this age. In the course of the survey, children should be offered the following types of assistance: the execution of an imitation action, the fulfillment of an imitation task with the use of pointing gestures, with speech instructions.
At the level of elementary imitation, the child can learn from an adult the way to perform one or another task, acting simultaneously with him. The number of hits on how to complete the task should not exceed three. In this case, the speech of an adult should serve as an indicator of the purpose of this task and evaluate the effectiveness of the child’s actions. Learning, i.e. the transition of the child from inappropriate actions to adequate, indicates the potential of the child. The lack of learning in some cases may be associated with a gross decrease in intelligence, with violations of the emotional-volitional sphere.
Normally developing children are characterized by interest in their activities and their end result. For a child with intellectual disabilities, indifference to what he does and to the result obtained is characteristic.
Features of development of children of preschool age.
At this age there are big changes in the entire mental development of the child. Its cognitive activity increases extremely - perception, visual thinking develops, the beginnings of logical thinking appear. The growth of cognitive opportunities contributes to the formation of semantic memory, voluntary attention.The role of speech significantly increases in the child’s knowledge of the surrounding world, as well as in the development of communication and various types of children's activities. Preschoolers have the opportunity to perform actions on verbal instructions, mastering knowledge on the basis of explanations, but only when they rely on clear visual representations.
The basis of knowledge for this age is sensory knowledge - perception and visual thinking. It is on how the perception of a preschooler child is formed, visual-effective and visual-figurative thinking that its cognitive abilities depend, as well as the further development of activity, speech and higher, logical forms of thinking.
New activities are emerging: the game is the first and main type of joint activity of preschoolers; graphic activity is the first productive activity of a child; elements of labor activity.
There is an intensive development of the child's personality. The development of the will begins. He learns moral ideas and behaviors in society.
By the end of preschool age, there is a readiness for schooling.
Features of the development of children of primary school age
The most characteristic for the period of 7-10 years is the transition to a new social status: a preschooler becomes a schoolboy.This is a transitional period, characterized by the fact that the child combines the features of preschool childhood with new qualities characteristic of the student.
During this period, the active maturation of all anatomical and physiological structures, the maturation of the nervous system continues.
The younger school age is characterized by the formation of a new type of activity — an educational activity, which requires from the child not only great mental exertion, activity, but also physical endurance.
The transition from play to learning activities significantly affects the motives and behavior of the child.
Quality learning activities will depend on how the necessary prerequisites were formed in the preschool period:
The overall physical development of the child, the state of vision, hearing, motility (especially the formation of small movements of the hands and fingers), the state of the child’s nervous system (degree of excitability and balance, strength and mobility). Disorders of nervous activity, as well as general health, primarily affect the child's performance, which can adversely affect not only academic performance, but also the student’s attitude to school, school, and communication with peers;
Mastering a sufficient amount of knowledge and ideas about the world, ideas about space, time, mastering elementary counting operations;
Mastering a clear, coherent, grammatically and phonetically correct speech, the ability to carry out the simplest sound-letter analysis;
The development of voluntary attention, mediated memorization, the ability to listen to the speech, the teacher's explanations, the ability to look and see, focus on work, remember what is needed to understand the new, the ability to explain, reason, draw appropriate conclusions;
Cognitive activity, desire to learn, interest in knowledge, curiosity;
Communicative activity, i.e. readiness for joint work with other children, cooperation, mutual assistance, ability to obey the requirements of adults.
On the basis of these prerequisites in the early school age, the formation of new qualities necessary for learning begins. It is during this period that very important psychological neoplasms appear, such as:
The arbitrariness of the activity;
The ability to plan their activities, the assessment of their actions in terms of compliance with the goals;
Mastering the skills of self-control.
In the process of educational activity, the child’s ability to distinguish properties, concepts when solving specific tasks, to master learning activities, control and evaluation. Formed skills volitional regulation of activity and behavior.
During the first years of school life, changes occur in the emotional and volitional sphere of the child. Gradually formed an adequate self-esteem, the level of aspirations, corresponding to the level of its development. His emotions become more stable, volitional qualities are produced. The most vivid expression of mental neoplasms is found in the development of cognitive processes. Perception develops: it becomes more focused and arbitrary. The volume of attention, the ability to concentrate, distribute, switch.
An important neoplasm in memory development is the transition to mediated memorization, mastering the techniques of memorization and reproduction.
Internal self-regulation and control begin to occupy a special place in mental processes.
The most important psychological neoplasm of school age is the transition to sign-symbolic activity. The use of graphic schemes, symbols in solving educational problems requires a sufficiently developed imagination and a qualitatively new, higher level of thinking.
If in the first class the visual forms of thinking continue to be the leading ones, then by the second or third year of study the child begins to carry out analysis and synthesis on the basis of ideas, mental comparison. There is a development of the verbal-logical form of thinking.
Conditions of prolonged deprivation significantly affect the formation of all these qualities: there is a delay in the psychophysical development of the child. There is a disharmony of development, which manifests itself in solving various psychological problems.
Limited social circle, poor life experience, some one-sided development (the predominance of formal verbal forms of education in the preschool years, the "organization" of children) does not contribute to the development of creative imagination and independence of judgment.
These and some other features related to the living conditions and upbringing of these children require special organization of examination and training.
Features of puberty
This period of development covers the age from about 10 to 15 years, coinciding in general with the education of children in middle school.AT adolescence there is a significant restructuring of the entire body of the child, which is reflected in mental characteristics. This is a period of rapid and at the same time uneven physical development, when there is increased body growth, the muscular system is being improved, the skeleton is ossified, but the intensity and duration of this process are individual.
Especially intensive is the growth of the skeleton and limbs in length, and the chest and pelvis lag behind in development, which creates the impression that the teenager is angular, inconsistent. This also causes some psychological manifestations - the teenager is aware of his angularity, hesitates her, tries to smooth out her inconsistency: she sometimes takes unnatural, fancy poses.
There is an age-related discrepancy in the development of the cardiovascular system. The heart significantly increases in volume, becomes stronger, works more powerfully, and the diameter of blood vessels lags behind in development. This often leads to some temporary circulatory disorders, increased blood pressure, cardiac tension, resulting in dizziness, palpitations, headaches, weakness, and relatively quick fatigue.
These features of the development of the cardiovascular system and the onset of intensive activity of the endocrine glands lead to some rapid disturbances in the nervous system of the adolescent: he may experience increased excitability, irritability, and short temper, which are sometimes expressed in a tendency to violent and sharp reactions such as affect. The nervous system of a teenager is not always able to withstand strong and long-lasting monotonous stimuli and, under their influence, often goes into a state of inhibition or, conversely, into a state of strong arousal.
During puberty, changes in coarse and fine motor skills occur, which leads to temporary impaired motor coordination, which is difficult and unreliable. Thus, the “eye-hand” interaction pattern formed in childhood loses its rigidity and must be re-established at a new level. However, the nature of the movements is affected by the relative inexperience of the adolescent in life situations, the overestimation of his own motor abilities, based on the unusually large body size, stiffness and uncertainty.
Puberty and psychosexual identity. The most important factor in physical development in adolescence is puberty. It begins in boys at 12–13 years old, in girls at 11–12 years old. Most boys mature in sex by age 15, and girls mature for age 13-14.
In the middle stage of puberty, many boys have a significant increase in the female-type breast, which usually disappears in about a year. Some boys are concerned about the insufficient, in their opinion, the size of the genitals.
Teenage girls are acutely experiencing skin defects (acne, acne), some tend to exaggerate their fullness, resorting to losing weight to unhealthy diets. If boys dream of increasing their height, then some girls would be happy to reduce it. If boys are confused by the lack of body hair, then girls, on the contrary, hair growth can cause panic.
With similar uncertainties of both sexes, physical changes in girls are often accompanied by shame, and in boys - by pride, since the latter associate them with sexual potency.
Natural and normal occurrence in adolescents in connection with puberty of sexual desire and relevant thoughts, feelings, experiences of a particular interest in the opposite sex, books, movies of relevant content. However, a real or imaginary delay in development, and premature maturation, fraught with too early sexualization of behavior, can lead to mental disorders.
In the process of puberty, the main neoplasm of puberty is formed - a sense of adulthood, when a teenager begins to believe that he is no longer a child, but becomes an adult, realizes his willingness to live in a team of adults as a full-fledged and equal participant in this life.
The sense of adulthood is the desire of adolescents to independence, which explains their sensitivity to the assessment of adults, touchiness, an acute reaction to the attempts of adults (real or apparent) to diminish their dignity, to reduce their adulthood. They want adults to reckon with their thoughts, feelings, and respect them.
The sense of adulthood is also manifested in the desire of adolescents to be relatively independent of adults, in the presence of their own views and judgments, in imitation of the appearance and behavior of adults.
Negative manifestations of adulthood are expressed in the fact that adolescents tend to resist the influence of elders, often do not accept their authority, ignore the demands made of them, are critical of the words and actions of parents and teachers.
Despite the fact that the body becomes sexually mature by the age of 13–15, this does not mean physical, and even more so, spiritual, social maturity at this age.
Features of cognitive processes and mental abilities of adolescents
Basis social situation development of a teenager is the fact that he is a schoolboy. The content and logic of the subjects studied in school, changes in the nature and forms of learning activities form and develop the cognitive processes and mental abilities of a teenager.Between the 11th and 15th years of life in the cognitive area there are significant structural changes, expressed in the transition to abstract and formal thinking. Thinking is less objectivity and visibility; it becomes possible to classify heterogeneous objects in accordance with arbitrarily selected criteria of a higher order.
It becomes possible to analyze any situation regardless of the real circumstances, the ability to systematically build and test hypotheses is acquired.
The object of thinking becomes not only the solution of externally assigned tasks, but also the process of its own thinking, i.e. thinking becomes reflexive.
An important mental neoplasm of adolescence is the development of the arbitrariness of all mental processes. A teenager can quite independently organize his attention, memory, thinking, imagination. He acquires the ability for complex analytical-synthetic perception (observation) of objects and phenomena. Perception becomes planned, consistent and comprehensive.
Significant changes undergo memory and attention. The ability to organize and control their attention, memory processes, manage them is growing. Significant progress is being made in memorizing verbal and abstract material. However, there are certain differences between boys and girls: girls usually surpass boys in verbal and speech activities, while boys excel girls in solving spatial problems and mathematical abilities.
At adolescence, attention development is characterized by a certain inconsistency: on the one hand, steady, voluntary attention is formed, on the other - an abundance of impressions, experiences, vigorous activity and impulsivity of a teenager often lead to instability of attention, its rapid distraction. Inattentive and scattered in one ("unloved") lesson, a student can work in a concentrated, concentrated way on another ("favorite") lesson.
The decline in performance often observed in high school, can be generated by various reasons - from minor gaps in knowledge or reduced performance related to age-related restructuring of the body and therefore of a temporary nature, until the onset of serious mental illness.
The most common cause of poor learning and difficulties in mastering a new situation of learning activities in middle school is the lack of adequate learning motivation, i.e. unwillingness to learn and imbalance of the positive and negative characteristics of the image of "I".
Such a form of self-affirmation as negativism, cynicism, clowning can be a protective psychological reaction to long-term trouble in educational activities and communication.
Despite structural changes in the cognitive domain, intellectual functions are not subject to dramatic "age shifts." Rather, there is a gradual development of trends observed in the previous phase.
Characteristics of the formation of personality
The main content of adolescence is its transition from childhood to adulthood. This transformation process defines all the basic personality characteristics of adolescents.Personality development goes in two ways: on the one hand, the process of personal maturation is gradual, not spasmodic, and emotional changes are not comparable with a sharp acceleration of growth or hormonal adjustment; on the other hand, despite growing up, a teenager retains important features and attributes of his personality. In contrast to intellectual functions, personality traits (especially those determining individual uniqueness) remain relatively constant both in the sphere of normal psychology and in the area of deviation from the norms of social behavior.
In adolescence, many needs arise for the first time or change. The needs of the teenager are:
Physiological needs. Among them stands out the desire for physical and sexual activity, for the appreciation of their physical development;
The need for security. Numerous biological and psychological changes, the consequences of which are difficult to assess in adolescence, reinforce this need. But security is not sought in the family, but in a group of peers;
The need for independence increases with the onset of maturity, the growth of cognitive abilities, and comes into conflict with parental constraints and expectations. Against this background, there are many family conflicts. The desire for independence conditions opposition to imposed opinions, denial of authorities, doubt in social norms, rules and customs;
The need for affection (love). Separation from the parental home, a feeling of confusion, a desire for independence and new cognitive abilities lead to a strong isolation of adolescents, which increases their need for love and affection. This is promoted by puberty and, as a result, the need for sexual activity, and at the same time, for tenderness and mutual understanding;
The need for success (achievement motivation). It is largely determined by the experience of early childhood. She is strong in those adolescents who are already used to succeed at preschool age, and during their school years (at the age of 8–10 years old) did not experience strict external control, which was replaced by their own striving for good results. In adolescence, achievement motivation can significantly weaken under the influence of the peer reference group;
The need for self-realization and development of their own "I", which means the manifestation of their abilities and their improvement. This need is largely correlated with the formation of a favorable self-image.
However, as the ability to self-analyze and self-esteem develops, a specific form of egocentrism may appear - "self-centered": "I am alone, no one understands me; I am unique, unique." Egocentrism of adolescents is manifested in another: they do not distinguish between reality and ideal ideas about it. Developing the ability of abstract thinking, analyzing one’s thoughts and thoughts of other people can lead to the emergence of a specific type of egocentrism (“imaginary audience”: “It seems to me that every outsider is watching me, and I am always on stage. I’ve never been alone with myself").
At the turn of the primary school and adolescence a self-assessment crisis occurs: often a decrease in self-esteem, a sense of self-worth. In fifth-grade boys, this crisis is more pronounced than in girls.
A generally high level of children's emotional-value attitude is being formed. However, in some it is combined with an adequate and critical perception of oneself as a subject of activity and communication, in others this relationship is combined with a “comfortable” interpretation of adverse factors, i.e. it is the result of connecting the defense mechanisms of the psyche. While resorting to self-deception, the child maintains a general positive attitude toward himself, but this circumstance makes it very difficult to advance in educational activities.
Intensive self-observation often leads to narcissistic crises and the so-called pubertal hypochondria.
The manifestation of these needs depends on the sex of the child. In girls, the need for security is more pronounced, they are weaker than boys, group orientation, fearfulness is stronger. Boys are less eager for safety, more focused on success and tend to obey the rules of a rigidly organized group.
For middle school students secondary school characterized by the development of volitional regulation of behavior - perseverance, perseverance in achieving the goal, in overcoming obstacles. At the same time, many of them, especially boys, manifest a conscious desire to develop volitional qualities. The teenager is already capable of volitional activity.
In adolescence, individual variability in emotional behavior is strongly pronounced. Moreover, the indicators of emotional stability in girls are lower than in boys, starting around 13 years old.
The development of values in adolescence is characterized by their complexity, depersonalization, increasing liberalism and increasing personal independence. Their content is continuously changing. A number of social values (help, self-sacrifice) temporarily lose their meaning; social status, authority, economic and ideological independence, hygiene and appearance are becoming relevant.
Adolescence is the most important period of character formation. If before it was possible to talk about individual characterological manifestations, then in adolescence the character gradually stabilizes and becomes stable. However, due to the peculiarities of physical development for a teenager, hesitant excitability is common, which in combination with vigorous energy and activity with insufficient endurance often leads to undesirable actions, violations of discipline, noisyness, restlessness.
In adolescence, dominant interests emerge, they often take the form of serious hobbies, a passion that captures schoolchildren, often at the expense of other, even very important, occupations.
Curiosity and curiosity, the desire to learn more, characteristic of adolescents, can generate the dispersion and instability of their interests. The presence of many interests at the same time, as well as frequent and unjustified change of them, usually leads to the satisfaction of superficial curiosity, the development of a light, frivolous attitude to different areas of life. However, in some cases, a teenager in this way (often unconsciously) gropes his central, core interest as the basis of his life orientation and tries himself in different areas. Some teenagers have professional intentions.
Personal psychological neoplasms of age:
The most important mental neoplasm of age is the emergence of a sense of adulthood during the process of puberty;
The arbitrariness of all mental processes;
Self-esteem as a regulator of behavior;
Reflexive nature of thinking;
Personal and interpersonal reflection;
From the very first days of his birth, a person begins, like a sponge, to absorb a huge amount of information coming from the external environment: from people, from things, from events and life situations. And besides the fact that a person begins to develop physically, his psyche, his personality is also formed. And hardly anyone will be able to give one hundred percent correct answer to the question of how this person will grow. But if you begin to understand what human development is, then you will find that this complex process has its own laws. And for this reason, one of the most important topics in psychology can definitely be called developmental psychology, to which this lesson is devoted.
In the process of studying the presented material we will get acquainted with the problem of development in psychology, as well as the subject and methods of developmental psychology and age psychology. Let us find out what specific questions developmental psychology studies, and what tasks it sets itself. Separately, we will talk about such things as the development of a child, the development of abilities. We learn what are the principles of development in psychology and how the formation and development of the personality occurs in general. In brief, we will touch on different age deviations and abnormal development.
What is developmental psychology
And according to our traditional scheme, to begin with, we need to understand what developmental psychology is in general, and how this phenomenon is understood in modern psychological science.
This is a field of psychology that studies a person’s psychological changes as he matures. Therefore, developmental psychology is often referred to as age psychology, although developmental psychology can be safely called the methodological basis of age psychology, since It contains a more extensive knowledge base. Developmental psychology may be part of developmental psychology, but in this lesson we will use these concepts as synonyms.
Developmental psychology includes several subsections:
- Prenatal and Perinatal Psychology - studies the mental life of unborn and newborn children;
- Child psychology - studies mental development child;
- Psychology of adolescence and adulthood - studies the mental characteristics of people in adolescence and adulthood;
- Gerontopsychology - studies the psyche of older people.
Developmental psychology is engaged in the study of the psyche and the human body in different age periods and at all stages. The emergence of developmental psychology dates back to 1882 and is associated with the publication of the book “The Soul of a Child” by the German psychologist Wilhelm Preyer. This work was devoted to child psychology. And in the 20th century, developmental psychology became an independent science. And like any serious independent science, developmental psychology has its own subject, object, tasks and functions, which we will discuss below.
Subject, object, tasks and functions of developmental psychology
The object of developmental psychology. Based on the fact that psychology is the science of man and his mental features, the object of developmental psychology is the person in the process of his development and maturation. Developmental psychology determines the changes in the psyche of people related to age, and tries to explain them, to understand the patterns by which people acquire knowledge and experience.
The subject of developmental psychology. The subject of study of developmental psychology are specific age periods, the reasons for transitions from one period to the next, and their mechanisms, trends, patterns, as well as the pace and direction of mental development in the process. common development person This also includes the individual and age characteristics of people, the development of mental processes and various types of activity, the formation of personality traits.
Tasks of developmental psychology. Developmental psychology has the following objectives:
- To uncover general patterns human development
- Establish the reasons for the transition from one stage to another.
- Categorize age periods
- Create a psychological picture of each period
- Examine the leading factors of development
In connection with the tasks, the following functions of developmental psychology can be distinguished:
- Descriptive function - describes the features of human development in specific age periods in terms of external manifestations and internal experiences;
- Explanatory function - explains and helps to understand the causes, factors and conditions of changes in a person’s behavior, as well as his experiences in different age periods;
- Predictive function - predicts certain changes in the behavior and experiences of a person at each age stage;
- Correction function - creates optimal conditions for managing human development.
Based on the foregoing, it can be concluded that age psychology reveals the psychological content of each stage of development (maturation) and their dynamics. Moreover, any changes are considered in the dynamics and taking into account the factors influencing the development of the human psyche. The research compares patterns of development at different stages, examines the mechanisms for acquiring and maintaining knowledge and skills, compares them, and further identifies factors that influence personal and intellectual growth.
In order to make it possible to compile the most objective and complete description of the development of the human psyche at all stages of his life, today in research a large number of different methods are used, which should be discussed in more detail.
Methods of developmental psychology
The developmental psychology uses general scientific and general psychological methods adapted specifically for it. And preference is given to the methods most suitable for studying age-related changes in the psyche and mental processes. All methods of developmental psychology can be divided into several categories: general scientific methods, psychogenetic, psychophysiological, historical and psychological. Consider each category separately.
General scientific methods
General scientific methods are a special modification of the methods used in many other scientific disciplines. Principal among them are observation, experiment and simulation.
Observation
Observation - this is a purposeful and regularly repeated study of a person, on the basis of the results of which an objective assessment is given. The method of observation is a prerequisite for other methods, such as journaling or autobiography. And the observation itself can be divided into several subspecies:
- Indirect observation (the researcher registers not the process itself, but only its result; such observation can occur through authorized persons);
- Direct observation (the researcher records the data under direct observation of the process);
- Field observation (the researcher records the data in the natural environment);
- Laboratory observation (artificial conditions are created specifically for observation);
- Open observation (the research is conducted openly and all its participants are aware of this);
- Covert observation (the object of observation may not be aware of the study or only a portion of the information is known);
- The included observation (the researcher himself participates in the process and can interact with the object);
- Non-included observation (the researcher can only observe, without becoming involved in the process itself);
- Accidental observation (the study is foreseen spontaneously, unplanned, due to the prevailing circumstances);
- Purposeful observation (the study is conducted on purpose, pre-planned);
- Continuous observation (the researcher observes all objects, not selecting anyone);
- Sampling observation (the researcher monitors a specific object);
- Arbitrary observation (uncontrolled observation that does not have a clear plan);
- Structured observation (the study is carried out on a specific plan, using special documents, instruments, etc.);
- Ascertaining observation (the study is conducted with the aim of recording data, without their evaluation);
- Assessing observation (the study is conducted with the aim of recording data and their evaluation).
You yourself can observe. It is only important to understand why you will spend it. Set a goal. This is the primary task. For example, you would like to know how easily your growing up child finds a common language with his peers. Use the method of purposeful non-included field direct observation. Simply put, when you go for a walk with your child, go to the playground and let him go to play, watch him, look at how he converges with other children. This kind of observation will give you the answer to the question that concerns you, you will know your child better, and also you can somehow improve the model of your upbringing in order to eliminate the shortcomings that have begun to manifest or, on the contrary, strengthen any positive qualities that you have noticed. Observation may be more scientific in nature if you define a specific goal, think carefully about your research plan, try to simulate a situation and create the necessary conditions, and also use any documentation to analyze or stick to a certain system.
Experiment
Experiment - it is a method of purposefully changing one or several variables and observing the results of this change. It differs from observation in that it studies the reactions of a person, and not the spontaneous manifestations of his psyche. There are several types of experiment:
- Laboratory experiment (the study is conducted under special conditions, and the subject knows about his participation);
- A natural experiment (the study is as close as possible to natural conditions, and the subject may not even be aware of his participation);
- Chamber experiment (the study is conducted in conditions less stringent than the laboratory, but not in the natural: room, special room, etc.);
- Formative experiment (during the study, the researcher is actively working on the subject);
- Individual experiment (research is conducted with one person);
- Group experiment (study conducted with a group of people).
The experiment is good because it can be carried out repeatedly and create special conditions to study the mental process of interest. For example, it is very easy to check under which conditions your child best assimilates the material being studied. Conduct such an experiment: find out your child's homework and in the first case give him the opportunity to perform it on his own, without helping him and not joining the process. In the second case, at run time homework stay close to your child and from time to time take part in homework (voice the task yourself or participate in the process itself). Such an experiment will allow you to find out which conditions are more suitable for your child to effectively perform homework and master the material being studied, and this, in turn, means that you will be able to create these conditions in the future, and your child’s performance can increase significantly.
Modeling
Modeling - this is the re-creation of a certain mental reality (state, situation, mood, etc.). The method of modeling is used in psychology in order to obtain more accurate data on the psyche of the person being studied, the peculiarities of his behavior in certain situations and under certain conditions, as well as his reactions to them.
Using the simulation method, you can find out, for example, whether your child has gotten rid of some bad habit after you have taken certain measures for this. Suppose you notice that your child constantly bites his nails when he has nothing to hold his hands for a long time. You told him that it was bad, in every possible way tried to show that it was not necessary to do this, that it was ugly and unhygienic, tried to distract him, so that the habit would fade into the background, they would use some other methods. Then you saw that the child didn’t chew on the nails for a week. In order to be convinced of the effectiveness or inefficiency of the methods you use to wean a child from a bad habit, you can specifically simulate a situation so that for a long time the child has nothing to hold his hands. Create conditions so that the internal impulses manifest themselves externally: stop distracting the child, turn on the cartoon or just leave it in the room, but so that there are no toys nearby, etc. of things. It is important that you can observe the child. See what he does, how his behavior has changed on a physical level. If your methods were effective, then you will see that the child will not bite his nails. If your methods were ineffective, then the child will again pull his hands to his mouth, and this will be an occasion to try to wean the child from the bad habit in some other way. Perhaps even contact a specialist in such matters.
The above examples of the application of general scientific methods, of course, are far from unique and not exhaustive. In fact, there are a lot of ways to use them and they all differ in their features. Our task is to understand the very idea and principle of work of general scientific methods. And for this you need to project them more often onto the surrounding reality and put it into practice.
Next on the list, but less important, are psycho-physiological methods.
Psychophysiological methods
Psychophysiological methods include methods of studying the higher nervous activity of children. The following are considered to be the most proven:
- Methods of studying conditioned reflexes, based on swallowing movements;
- Method of studying conditioned reflexes, based on grasping movements;
- A technique for studying conditioned reflexes, based on tentative reinforcement (for example, the appearance of a picture);
- Methods of studying conditioned reflexes, based on verbal reinforcement;
- Methods of research sucking food reflexes;
- Methods of research defensive defensive eye movements;
- Replacing the immediate stimulus with its verbal designation
Psychophysiological methods are usually used to study children in the first and second year of life and in specialized institutions. Therefore, if you are not a narrow specialist, these techniques are unlikely to give any results or practically valuable knowledge. The most convenient and recommended way to become familiar with psycho-physiological methods is to observe how they are used by experts, as well as the ability to correctly interpret the data.
Psychogenetic methods
Psychogenetic methods are aimed at isolating environmental and heredity factors in individual variations of psychological qualities. It can be said that “genotypic-environmental” is being studied, where a genotype is a set of genes, and a medium is non-genetic factors influencing a person. The main psychogenetic methods are:
- The twin method based on a comparison of two types of twins (monozygous, developed from one egg and dizygotic, developed from two or more eggs). There are also variations of the twin method: the classical, the control twin method, the separated twins method, the family method, etc .;
- Method of foster children;
- Pedigree analysis method (genealogical).
Psychogenetic methods, along with psycho-physiological, can be used only by specialists and in specialized institutions, since seem to be the most complex and require a purely scientific approach.
Historical methods
Historical methods, or, as they are also called, methods of analyzing documents, study the life course of a person, features of heredity, and the environment that created special prerequisites for his spiritual formation. Generally, historical methods study those people whose activity had or has a certain cultural value, but can also be used to study the lives of ordinary people. This group of methods includes the following:
- Diary
- Autobiographical
- Biographical
- Pathographic (describes the disease of prominent people)
Historical methods seem to be very convenient for use in practice even by ordinary people. If you have some person who admires you, and you would like to know more about him, his life, the conditions in which he developed, his inner world, you can use the biographical or autobiographical method. To do this, you need to find and get acquainted with the sources that contain data about the life and personality of this person. And if you want to identify any patterns or important stages in the development of your child, you can use the diary method. Keep a diary of your observations regarding the subject of study. This diary should be a kind of observation protocol, the analysis of which will help reveal what you need. By the way, the diary method is very popular and many psychologists have created their theories based on observations of their children.
And the last group of methods of developmental psychology are psychological methods.
Psychological methods
Psychological methods can be divided into two subgroups.
TO the first subgroup include introspective methods. They are designed to directly collect information about the object of study. Here stand out:
- Introspection - it is used to reveal certain features and mental phenomena of a person to himself;
- Self-esteem - used to identify a person with himself not only features and phenomena, but also stable mental qualities.
To the second subgroup are the socio-psychological methods, carried out, in most cases, indirectly. Here stand out:
- Conversation - obtaining information through communication, where the roles of the participants are equal (the conversation of the teacher and the student, the conversation of father and son, etc.);
- Interview - receiving information through communication, where one person asks questions, is a leader, and the second answers, is a slave (oral exam, etc.);
- Questioning - obtaining information through the answers of people to the prepared questions;
- Sociometry - obtaining information through the study of the status of a person in society (a group of people);
- Analysis of the products of activity (creativity) - obtaining information through the control of knowledge (dictations, essays, etc.), the restoration of activity from the opposite (from the result), graphics, drawings, etc .;
- Testing - obtaining information through brief structured tests (ability tests, perception tests, skills tests, projective tests, career guidance tests, intellectual tests, etc.).
Psychological methods can be safely ranked as the most frequently used in developmental psychology. One of the reasons for this is the convenience of their use and the ability to apply almost everywhere. You yourself can use any of the psychological methods to learn more about yourself or your loved ones. For yourself, for example, you can use the method of self-observation, which will help you learn more about the characteristics of your character, habits, reactions, etc. If you have a child, you can offer him a few tests. The determination of what the test will be designed for is up to you. A huge number of various tests you can find on the Internet or in special collections that are sold in bookstores.
You can get more information about psychological methods from the second lesson of this training.
Research methods in developmental psychology exist, as we have already noticed, quite a lot. And for the most accurate determination and study of the origin, occurrence and development of mental manifestations of a person at each stage of his development, these methods should be used, both separately and in combination. But what is no less important is to take into account the age of people whose psyche features are being studied, because there are certain age groupswith their own special characteristics and features. About what age groups are, we will tell below.
Age groups
![]()
Age - this is a peculiar period of physical, psychological and behavioral development, which is characterized by its features. There are several kinds of ages:
- Biological age - the degree of development of the organism;
- Social age - the degree of development of social roles and functions;
- Psychological age - features of psychology and behavior;
- Physical age - quantitative indicator of human development (days, weeks, months, years).
The division of a person’s life path exists in order to allow a better understanding of the patterns of development and the specifics of different age stages. Attempts to periodize the entire history of developmental psychology have been made. But the problem is objective age periodization remains relevant to this day, because none of the previously proposed periodization was confirmed in the specific results of the study of developmental psychology. But, of course, despite this, the main age groups can still be distinguished. Best for this periodization is suitable for physical grounds:
- Infancy (from birth to 1 year)
- Early childhood (from 1 year to 3 years)
- Preschool age, playing (from 3 to 6 years)
- School age (from 6 to 12 years)
- Youth (from 12 to 20 years)
- Youth (from 20 to 25 years)
- Adulthood (from 25 to 60 years)
- Old age (from 60 years)
Each age group, among other things, is characterized by its psychological features. And the psychological periods do not coincide with the physical periods indicated above. So, if we consider the age groups on a psychological basis, the picture will look like this:
Up to 1 year
Everything here is extremely simple: the main thing that parents need to do in order for a child to develop is to support his livelihoods, feed, care, etc. It is during this period that the child begins to learn about the world around him. Even at such a small age, a person’s character, behavior, and perception begins to manifest. You need to be careful and pay attention to absolutely everything related to the child.
From 1 to 3 years
During this period, the situation changes, the child begins to walk, to show interest in his body and his genitals, and also to expand his, so far small, vocabulary. The individuality of the child begins to manifest itself and it is already possible to begin to notice its differences from other children. You can also see manifestations of predisposition. For example, you can give your kid a marker and see what he will do with him: he will begin to nibble, throw, or draw. Try to watch him more - it will help to identify any tendencies or, on the contrary, deviations.
3 years
This period is associated with a crisis of 3 years, because from a calm baby, a child turns into a capricious fidget, begins to argue with parents, roll up scandals, etc. This is the period when you need to learn how to find points of contact with your child, negotiate with him, develop your tactics of behavior and manner of education. At this age, you can already give the child in kindergarten. But before you do this, you should determine whether it will benefit him or not. To make it easier to do, and indeed, to find an approach to the child, study more specialized literature, apply knowledge in practice. It may be worth attending several seminars on raising young children. And, of course, continue to monitor the child and use different approaches in communication and upbringing. By the method of experiments, trial and error you will find the best option.
4 years
The next stage of changes in the psychology of the child: he begins to be more actively interested in the surrounding world and more consciously perceive information. Therefore, it's time to think about what information comes to your child, what he watches on TV, what books you read to him, what you talk to him about. Best of all, if you supply it with only useful and developing information, you will begin to learn to read and write letters. Read good tales and stories to him, try to keep him from watching scenes of violence on television, senseless TV shows and stupid cartoons. In general, bring to the child only the information that will contribute to its development.
5 years
This period in the development of a child is characterized by the fact that he begins to be interested in the causes of various phenomena, and more and more often he asks why these or other things happen. Many children at this age have different kinds of fears, they are worried about some phenomena and events, nightmares can happen. At this stage, you should focus your attention on the manifestation of such moments. Be interested in what bothers your child, what makes him worry and worry. Watch how he expresses his concerns. It can be pictures, strange inscriptions, unusual behavior. Pay attention to how you behave yourself in the process of ordinary life, communicating with him and other people. In this period, the transition of the perception of your child from his previous perception of various phenomena to a more meaningful one is possible.
6 years
At this stage in the development of a child, you may notice that there are prerequisites for the concept of what sexuality is. Many parents are shocked by the fact that their children are beginning to talk about indecent things, use obscene expressions in their speech. It is important to determine whether this is the norm or deviation. The child may be asked questions about how they came and where children come from. At this stage, you need to be able to adequately explain such things to your child in order for him to form correct judgments and ideas about issues relating to sensitive topics.
7-11 years old
At this age, the child goes to school, and this event has a huge impact on the development of the younger person. This age is often called the top of childhood. In the psychology of the child there are many new landmarks, which are teachers, as well as assessing their performance. In spite of the fact that at this age, the child tends to retain many children's qualities (naivety, frivolity, orientation to adults), he begins to lose in behavior the childish spontaneity inherent in him, new thinking patterns appear. Learning is a significant activity, because new knowledge, skills, skills, social status are acquired, interests and values change, as well as lifestyle. At this stage, it is important for the parent to pay special attention to his child, talk more with him, discuss his affairs, successes and failures, be able to cheer up, set him on the right path, set up in a positive way. It plays a very important role in its subsequent development and perception of the others and of itself.
12-16 years old
This stage in the development of a teenager is characterized by intimate-personal communication with peers, a sense of adulthood, critical thinking, a need for self-affirmation, self-centeredness, and an increase in self-awareness. A teenager at this age is looking for himself, trying to show his individuality in appearance, manner of behavior and speech. Vividly expressed desire for self-education and self-development, the need for communication, independence and independence from adults, emotional instability, the adoption of moral values, the fickle behavior, instability of attitudes and actions. It is very important to be attentive to what your child does in his free time, what he is interested in, who he communicates with, who he is friends with, and whether he has relationships with adolescents of the opposite sex. If you notice your child’s aggressiveness towards you, frequent mood swings, reduced desire to learn, absenteeism, indifferent attitude to requests, antisocial behavior, etc., then you should use special methods of communication. Namely: to build communication on the basis of respect and goodwill, to accept refusals and discuss necessary to carry out the case, be able to justify their point of view, more often spend time together, take part in the teenager’s personal life and be interested in his hobbies, control studying proccess, to conduct confidential conversations, to give the opportunity to freely communicate with peers, to make recommendations about internal and external expression. This strategy will allow you to set up a positive line in controlling the development of your child, to find common ground with him and to achieve success in mutual understanding.
16 years old - 22 years old
At this age, adolescents are increasingly seeking to show and prove their readiness for adulthood and independence. The greatest difficulty here is that the teenager is already an independent person and a person who still needs help and care. This is the time of youthful maximalism, as well as fatalism, in which the loss of hope for a bright future, the futility of being, aspirations and life itself can be traced. During this period, you need to give your child even greater support, although all the circumstances suggest otherwise. You can not go on about the teenager and bend under his pressure. It is important to choose a specific demeanor so that the person does not feel hurt and is not hurt and, at the same time, you can make sure that he can adequately accept support and advice from your side.
23 years old - 28 years old
This period of human development is characterized by the search for oneself, the awareness of one’s individuality, the formation of oneself as an adult with his rights, abilities, duties, obligations. A special place is occupied by the thoughts about what place a person should take in life, what he aspires to, where to go, in which direction to develop. Here it is important and you need to be a mentor, to direct, support, advise, conduct the right conversations, etc. If you do not have the proper influence, then factors that play an important role in the previous age group can affect development.
29 years old - 32 years old
This period can be characterized as transitional, since Many of the ideas, attitudes and beliefs that were formed earlier are often incorrect, and life itself no longer seems as rosy and simple as it seemed before. At this stage, questions arise about the meaning of life, the correctness of the chosen path, the activities in which a person is engaged, his beliefs and worldview. Often, people at that age destroy the foundations of their past, change their lifestyles, realize new truths, set new goals for themselves and strive for them. The most fruitful work in this period is the work of a person on himself, his self-awareness, world perception, awareness of true values.
33 years - 39 years
At this stage of life, a person experiences pleasure from the activity in which he is engaged, strives for career growth, achievement of success and all related benefits. The main thing here is that a person must be 100% sure of the correctness of the chosen direction and should not have any doubts in the choice of his life path. Otherwise, a person can be overcome by depression and psychological crisis, which can be eliminated either by careful and scrupulous work on oneself, or by the help of a qualified specialist.
40 years old - 42 years old
The time of the critical period. What a person has achieved seems to him insignificant and insufficient, there is often a feeling that life is wasted, nothing makes sense, health and strength are declining, youth has passed, etc. As in the previous period, further psychological development depends on the person’s self-perception, his picture of the world and the presentation of his place in it.
43 years old - 49 years old
The new period of equilibrium, which is characterized by stability of the psyche, beliefs, worldview. A man with new forces is ready to work, especially if it is some kind of new activity, creative people experience a rush of inspiration. Everything contributes to living harmoniously and purposefully. It is very good if a person at this age feels support from relatives and friends, feels his need, the participation of other people in his life.
After 50 years
After 50 years, people tend to come to a more harmonious life. They are in harmony with themselves, have a rich life experience and can give an adequate assessment of their way of life, past, present. The man already knows himself well. Often there is a desire to know things of a higher order, the meaning of being, the causes of everything that happens. But this is done not from the position of the victim of meaningless existence, but from the position of a mature personality, a mature person. A person who is over 50 may also feel the need to communicate with people. Often, old connections are established and maintained, and new ones appear. The best conditions for a normal life during this period are comfort, tranquility, a safe atmosphere, confidence in the future, the knowledge that there are close people who can always help and support.
As you can see, each age group has its own characteristics and properties. Mental differences at each stage of human development affect his behavior, perception, activity, social activity and other important properties of his personality. Knowledge of age groups and their features are of practical importance, since They can be used to better understand your loved ones, just people around themselves and themselves. With this knowledge you can always find the best approach to a person of any age and make communication with him more productive, and life calm and harmonious.
In addition to the fact that there are different age groups with their own properties, there is another important topic that you should be aware of in order to be able to get an objective idea of the psychology of human development. These are factors that influence development.
Factors affecting human development
The development of a person, his worldview, interests, needs, orientation of his actions, spiritual wealth of his personality and other features are directly dependent on what conditions he develops and, especially, during the period of childhood and adolescence. The personality of a person is formed under the influence of a number of factors. The main among them are the following three: heredity, environment and education. And they, in turn, can be divided into two large subgroups: biological (heredity) and social factors (environment, upbringing).
Heredity
Heredity - this is information embedded in the human genes and transmitted from parents to children. And it consists of two parts:
- Constant part (ensuring the birth of a person by a person)
- Variable part (what binds a person and his parents)
Once a person is born, he is not yet a person. His “I” has not yet manifested, he has no name, ideas, views, tastes, beliefs, morals, social status, etc. We can say that his life path is still unknown, and fate is not predetermined. But in how a person develops, heredity plays a big role. A person with better heredity will successfully develop in society and interact with the outside world. An important condition is that a person born with certain characteristics will develop only within their framework. Thus, it turns out that the person is who he is, and his hereditary characteristics will affect him throughout his life. In fact, it looks like the fact that a person born with poor physical heredity cannot achieve outstanding results in sports and physical activity, and the one born mentally retarded will never become a scientist, a philosopher, etc.
More information about heredity can be found.
Wednesday
Under by medium one can understand natural, climatic, etc. conditions in which a person develops; state system, culture of the people, its traditions, customs, life. But also, the medium is directly understood as the society in which a person develops: family, microclimate in the family, relations between parents, the subtleties of upbringing, friends, classmates and other people around.
The way in which a person develops has an impact on his socialization, the formation of knowledge, skills, behavior, social norms, attitudes towards culture, learning, work, and other people. In the environment are made out psychological characteristics rights, needs, attitudes, interests, aspirations, personal, social, political, ideological and material values. For example, a person who grew up in a dysfunctional family, raised by alcoholic parents, communicated with children from other similar families, will have values and aspirations that are different from the values and aspirations of a child who grew up in prosperity, brought up by cultural people (teachers, people of art, scientists) If you have a child and you want to grow it as a worthy person, you should definitely monitor the environment in which it grows and develops. In your hands to create the environment in which the development will be the best. You can also conduct a small experiment about the influence of the environment on human development and experience the result by example. Try changing your social circle. Not forever, but for a while - for the sake of experiment. If you are dominated by people accustomed to complaining about problems, complaining about their lives, blaming everyone for their failures, you can begin to communicate with people who are successful, self-confident, goal-oriented, self-confident and accustomed to manage their own lives. Literally after a month of being in a new environment, you will see how your beliefs, attitudes, reactions, and aspirations began to change. Your old friends will appear before you in a completely different light. This is one of the examples of the influence of the environment on humans.
You can learn more about what the environment is and its impact at this link.
Upbringing
Upbringing - it is a purposeful formation of personality, preparing it for life in society. This factor is somewhat different, in contrast to the previous two, the character - focus and awareness. Another feature of education is that it always occurs in accordance with the sociocultural values of the society in which it is carried out.
Under the upbringing almost always refers to positive effects, and systematic, since single impacts do not bring results. As a rule, the parents of the child are the main ones in the process of upbringing, the secondary roles are played by educators, teachers, teachers, etc. Parents pass on knowledge and life experience to their children, teach them things, explain, show, tell, control. The way he grows up, how he will communicate with other people and behave in society, what moral and ethical standards, beliefs, and so on will depend on what kind of upbringing was given to the child. In order to make a real person out of a growing up child, it is necessary to make great efforts to correct upbringing. This applies to everything from small to large: from the fact that it is uncivilized and unhygienic to nibble at the nails and to the fact that you need to remove the headdress in the room; from the fact that you do not need to swear and to the fact that you should have a goal in life and something to strive for. Examples can cite many. But what is more important is to understand the mechanisms of influence on the child. Now a lot of literature on parenting has been written, some trainings and seminars on this topic are constantly held, there are many websites on the Internet specializing in educational counseling. Use different sources, apply knowledge in practice and be attentive to your children. But remember that the main thing in upbringing is your own example, because a child will probably someday want to smoke a cigarette, even if his parents say it is bad and they smoke themselves.
You can get acquainted with not less interesting information about education by following this link.
The factors, under the influence of which the personality is formed, do not have their influence alone, but in a complex, i.e. together. For this reason, when studying the psychology of human development, it is necessary to take into account any details, nuances, events and phenomena that a person encounters in his life path. Only such an approach will provide an opportunity to understand why a person (in any plan) was formed that way, and not otherwise.
Everything that we have considered in this lesson is an integral part of the development of a person and his life. Every person is a unique creation, formed under the influence of many factors, and this process obeys its own laws. Developmental psychology, or to be more precise, knowledge about it is the key to successful understanding of your children, parents, relatives, friends, yourself and the person in general. Using the knowledge gained in our everyday life, we can make our lives better, more successful, more harmonious and happier, and always reach an understanding with people nearby!
Literature
If you want to get acquainted with the topic of developmental psychology in more detail and learn even more interesting and useful information, you can use the list of references that we have provided below.
- Abramova G.S. Developmental Psychology: Textbook. manual for university students. - M .: Academy, 1997
- Abramova G.S. Psychology of human life: Studies of gerontopsychology: Proc. manual for students psychol. fact universities. - M .: Izd. Center "Academy", 2002
- Bern E. Games that people play. Psychology of human relationships Publisher: Eksmo, 2008
- Vasilyeva T.V. You understand me? (Tests for children 5-7 years with the recommendations of the psychologist). - S.-Pb, 1994
- Wilson G., Grylls D. Learn your child’s IQ M., 1998
- Vygotsky L.S. Questions of child psychology. - S.-Pb. - 1999
- Gamezo M.V., Domashenko I.A. Atlas of psychology. - M., 2003.
- Craig Grace. Developmental psychology. - S-Pb, 2000
- Kulagina I.Yu. Developmental psychology: the development of a child from birth to 17 years. - M., 1998
- I. Yu. Kulagina, V. N. Kolyutsky. Developmental Psychology: Human Development from Birth to Late Maturity: (Full Human Development Life Cycle): Proc. manual for students of higher spec. educational institutions. - M., 2001
- Craig Grace. Developmental psychology. - SPb, 2000
- Mill J. On Freedom / Trans. from English A. Friedman. Science and life. -1993.№11
- Mukhina V.S. Developmental psychology: phenomenology of development, childhood, adolescence. - M., 1999
- Orlov, Yu. M. Ascent to individuality: Book. for the teacher. - M .: Enlightenment, 1991
- Obukhova L.F. Age-related psychology. - M., 2000
- Social philosophy. Textbook. - Edited by I.A. Gobozova. - M .: Publisher Savin SA, 2003
- Sorokin P. A Man. Civilization. Society / Society ed. and foreword A. Yu. Soghomonov: Trans. from English - M .: Politizdat, 1992
- Uruntaeva G. A. Preschool psychology: Proc. manual for students of secondary ped. educational institutions. - M .: Izd. Center "Academy", 1999.
Test your knowledge
If you want to test your knowledge on the topic of this lesson, you can take a small test consisting of several questions. In each question, only 1 option can be correct. After you select one of the options, the system automatically proceeds to the next question. The points you get are affected by the correctness of your answers and the time spent in passing. Please note that the questions are different each time, and the options are mixed.
Introduction Healthy child
"... and that's when they asked to bring the most beautiful thing in the whole wide world, the crow brought her child ..."
The first fragmentary information about a healthy and sick child appeared in ancient times. Hippocrates, Galen, Soran, Avicenna emphasized in their treatises the presence of features of a children's organism that distinguishes it from an adult and determines the atypical course of diseases, especially in early childhood. Even then, scientists paid much attention to the importance of breastfeeding, physical education and proper care for the harmonious growth and development of the child.
Russian scientists have made a huge contribution to the development of national pediatrics. N.F. Filatov - the founder of domestic pediatrics, N.P. Gundobin, the author of the classification of periods of childhood, and other scholars, in their works, singled out sections on healthy children, feeding and upbringing.
In the modern world, time needs to be given great attention to the development and upbringing of children, since children are the future of our planet.
1. Periods of childhood
The body of the child all the time is in the process of growth and development, which occur continuously in a certain regular sequence. From the moment of birth to an adult, a child goes through certain age periods.
A child in different periods of life is characterized by certain anatomical and physiological features, the totality of which affects the reactive properties and body resistance. This explains the peculiarity of the pathology, and the peculiar course of certain diseases in children of different age groups.
But we should not think that the age characteristics of the child themselves doomed him to the disease. If the environmental conditions, temperature, nutrition, care, use of fresh air, etc. meet the requirements of the body of a newborn or infant, then this creates the prerequisites for its proper growth, development and protection from diseases. Conversely, adverse environmental conditions adversely affect the health of the child. Even small errors in care, nutrition, and temperature can adversely affect the health of a child, especially a newborn and an infant.
The most acceptable for practical purposes is the N. N. Gundobin scheme, according to which the entire childhood age is divided into the following periods.
Gundobin Nikolay Petrovich, Russian pediatrician. He graduated in 1885, medical faculty of Moscow University. Since 1897 Professor of the Department of Children's Diseases of the Military Medical Academy in St. Petersburg. The main works are devoted to the study of the age characteristics of the anatomy, physiology and pathology of the children's body. Gundobin N.P. He was chairman of the school department of the Society for the Conservation of Public Health and one of the organizers (1904, together with N. A. Russkikh) of the Union to Combat Child Mortality.
Cit .: The education and treatment of a child up to the age of seven, 3rd ed., M., 1913; Features of childhood, St. Petersburg, 1906.
I. The period of prenatal development: 1) the phase of embryonic development (embryo), 2) the phase of placental development (fetus).
Ii. The neonatal period.
Iii. The period of infancy (younger nursery),
Iv. The period of milk teeth: a - preschool age (older nursery), b - preschool age (period of attendance at kindergarten).
V. The period of adolescence (primary school age).
Vi. Puberty (senior school age).
In parentheses are marked all the changes that have been made by Soviet pediatricians.
This division is conditional, and it is rather difficult to draw clear lines between periods. But they are convenient to use when studying the physiological and pathological conditions of the child, as well as for practical therapeutic and preventive purposes.
2. Stages of intrauterine development
In prenatal human development, there are conventionally three periods:
The implantation period lasts from the moment of fertilization to 2 weeks. This period is characterized by rapid systematic fragmentation of a fertilized egg, its promotion through the fallopian tube to the uterus; implantation (attachment of the embryo and introduction into the uterine mucosa) on the 6-7th day after fertilization and further formation of the fetal membranes, creating the necessary conditions for the development of the embryo. They provide nutrition (trophoblast), create a liquid habitat and mechanical protection (fluid of the fetal bladder).
The embryonic period lasts from the 3rd to the 10th-12th week of pregnancy. During this period, the rudiments of all the most important organs and systems of the future baby are formed, the body, head and limbs are formed. The placenta is developing - the most important organ of pregnancy, which separates the two blood flows (mother and fetus) and ensures the exchange of substances between the mother and the fetus, protecting it from infectious and other harmful factors, from the mother’s immune system. At the end of this period, the embryo becomes a fetus that has a childlike configuration.
The fetal period begins with the 3rd month of pregnancy and ends with the birth of a child. Nutrition and metabolism of the fetus through the placenta. There is a rapid growth of the fetus, the formation of tissues, the development of organs and systems from their buds, the formation and formation of new functional systems that ensure the life of the fetus in the womb of the mother and child after birth.
After the 28th week of pregnancy, the fetus begins to form a reserve of valuable substances needed during the first time after birth - salts of calcium, iron, copper, vitamin B12, and others. Maturation of the surfactant, which provides normal lung function, occurs. Fetal development is affected by various environmental factors. They have the most significant effect on the organs that develop most intensively at the time of exposure.
3. Thoracic period
The chest period - from 4 weeks to 1 year of life - is characterized by an intense increase in body weight and height, by intense physical, psychological, intellectual development. By 4 months, body weight doubles, and by 1 year - tripled.
For the first quarter of the year, the child grows monthly by 3 cm, for the second quarter - by 2.5 cm, for the third quarter - by 1.5 cm and for the fourth quarter of the year, the child each month adds 1 cm to his height. big changes in the psychomotor development of the child, during this period the foundation of health, physical and mental development was laid. It is estimated every quarter of the year.
In the development of the visual analyzer, the following occurs: by the end of the 1st month, visual concentration is observed; k 2 - 3 rd month - fixing the gaze with simultaneous reactions of the muscles of the neck and head; by 3.5 months - distinguishing surrounding objects, prolonged concentration, tracking of objects; by 5 months, the ability to view an object at close range is manifested; for 6 months, the child clearly distinguishes colors, expressing a definite relationship to them.
Reactions of the auditory perception are manifested, in addition to auditory concentration (end of the 2nd week), a clear orientation to the sounds (1st month) and the search for its source from the end of the 2nd month. In 2-3 months, the child listens to sounds, and in 3-3.5 months, he unmistakably finds the source of the sound. In 3-7 months, there is a constant activity on various sound stimuli, and from 10-11 months - a reaction to the sound in connection with the content and meaning of this sound.
The development of the child’s motor skills - keeps the head, if you keep it upright (at 5-6th week), lifts the head or turns it to the side in a position on the stomach (at the 5th week), turns over on its side from lying on back (4-4.5 months), sits independently (6-7 months), walks on all fours (at the 8th month), stands up and stands, adhering to the support (7-8 months), walks independently (at 11-12 month).
Development of grasping ability - stretches a hand to the object (at the 3rd month), seizes the object (4.5 months), holds the object in each hand (6 months), brings the whole body to the active state when grabbing (at the 7th month), the beginnings of specific manipulations (on the 11th month).
Teething from 5-7 months.
From 4-6 weeks, visual-auditory search and visual concentration on the adult's face are observed, and from 3 months there is a pronounced need for communication with adults. In an infant, the leading line of physical activity at 7-8 months is crawling, at the 12th month - the beginnings of manipulation games.
The development of the I and II signaling systems of the central nervous system, the thymus and thyroid glands are functioning; adrenal function weakened; start of pituitary function.
Rachitis, dystrophy, food and respiratory allergies, respiratory diseases and acute gastrointestinal diseases can occur.
In each period for the proper development of the child requires the creation of certain environmental conditions, regime, education.
Features of growth and development
Significant growth rates are characteristic - body length (growth) increases by 50% at birth, reaches 75-77 cm by 1 year. Head circumference is 46-47 cm by year, breast circumference is 48 cm. Motility develops rapidly and motor skills. Three peaks of motor activity are distinguished: I - 3-4 months - a complex of revival, joy at the first contact with adults; II - 7-8 months - crawling activation, formation of binocular vision (mastering the space); III peak - 11-12 months - the beginning of the walk. Their sensory-motor connections are determined. Skeletal muscles and physical activity are the factors determining the processes of growth and development in the first year of a child's life. The growth rate is ensured by a high metabolism.
Features of the central nervous system
An increase in the brain mass by one year is 2-2.5 times, the most intensive differentiation of nerve cells in the first 5-6 months of life. Not enough activity-aminobutyric acid (inhibitory factor) and little myelin, which contributes to the rapid spread of any excitement.
An approximate reflex is maintained, reflecting the innate need for movement and the activity of the sense organs. Nervous connections between the child and surrounding people are established through facial expressions, gestures, and voice intonations. The development of subtle hand movements contributes to the development of brain and speech. There are connections between the words and the response motor responses of the child, then the child connects the visual and auditory perception of objects with the words, the names of the objects when they are shown, and links with individual actions (“give”, “show”) - this is the optimal course of development necessary as basis for other periods of childhood. The need for contact with adults determines the mental development of the child.
Electroencephalogram in 2-3 months - steady rhythm; in 4-6 months - changes are unidirectional; in 8-10 months - progressive individualization.
Features of the endocrine system
In the thoracic period, there is an increase in the function of the pituitary and thyroid glands. They stimulate the growth and development of the child, metabolism, provide normal differentiation of the brain and intellectual development. Adrenal function is enhanced, partial involution of the adrenal fetal cortex occurs, and the biological activity of corticosteroids is increased.
Immunity Features
There is a slight decrease in the number of T and B cells in the blood compared with the neonatal period. The reduction of maternal IgG from 2-3 months is expressed, the synthesis of its own IgG increases from 2-3 months; its constant level is established after 8 months - 1 year. The level of IgM by the end of the year is 50% of the adult level. The concentration of IgA slowly increases. IgE in a healthy child is contained in insignificant amounts, its level depends on the manifestations of allergy (increases). The second critical period of immunity is noted at 4-6 months and is characterized by: the lowest level of specific antibodies - physiological hypogammaglobulinemia; synthesis of IgM antibodies that leave no immunological memory. An atypical flow of measles, whooping cough - leaving no immunity! High sensitivity to respiratory syncytial infection, parainfluenza viruses and adenoviruses remains.
Non-specific resistance factors
Typically high levels of lysozyme and properdin. By the end of the first month of life, the level of complement rapidly increases and reaches the level of an adult. From 2-6 months the final phase of phagocytosis of leukocytes to pathogenic microorganisms, with the exception of pneumococcus, staphylococcus, Klebsiella, hemophilus bacilli, is formed.
Nature of pathology
Often develop respiratory diseases, acute gastrointestinal diseases, food allergies, rickets, degeneration, iron deficiency anemia. Possible manifestation of hereditary diseases, tuberculosis, syphilis, HIV infection.
Assessment of physical development, motor skills, speech development, neuropsychic development, taking into account the leading line of development in the thoracic period, is carried out quarterly.
To assess the physical development of children under 1 year old it is better to use the following indicators:
Body mass;
Proportionality of development (head circumference; chest circumference, some anthropometric indices);
Static functions (motor skills of the child);
Timely eruption of milk teeth (in children up to 2 years).
The skull of a newborn has specific features. See fig.
The most stable indicator of physical development is the growth of the child. It determines the absolute length of the body and, accordingly, the increase in body size, development, maturation of its organs and systems, the formation of functions in one or another period of time.
The highest growth energy is in the first quarter of the year (Table A). In full-term newborns, growth ranges from 46 to 60 cm. On average, 48-52 cm, but adaptive growth rates are considered to be 50-52 cm. This means that adaptation in the prenatal period occurred not only at the organism level, but also at the organ level and enzymatic.
Table A. Increase in height and body weight in children of the first year of life
Age, months | Growth gain for the month, see | Growth over the past period, see | Monthly weight gain, gr. | The increase in body weight over the past period, gr. | |
During the first year, the child grows an average of 25 cm in height, so that by the year his height averages 75-76 cm. With the right development of the child, the monthly increase in growth can vary within ± 1 cm, but by 6 months and by the year these fluctuations height should not exceed 1 cm.
Growth reflects the characteristics of plastic processes occurring in the human body. Hence the importance of high-quality nutrition, especially the content of a sufficient amount of a balanced full-fledged protein component and vitamins of group B, as well as A, D, E. Certainly, the “gold standard” of optimal nutrition for children under 1 year old is breast milk. The deficiency of some food components selectively disrupts growth in children. These include vitamin A, zinc, iodine. Growth can be caused by various chronic diseases.
Growth measurements for a child in the first year of life are made on a horizontal stadiometer. Measurements are made by 2 people. Measuring is on the right side of the child. The helper keeps the child's head in a horizontal position so that the upper edge of the ear trestle and the lower edge of the orbit are in the same plane perpendicular to the height plate. The apical part of the head should touch the vertical fixed bar. The arms of the child are extended along the body. Measuring with a light pressure on the child's knees with his left hand, he holds his legs in a straightened position, and with his right hand pushes the moving bar of the height meter tightly to the plantar side of the feet, bent at a right angle.
In the second year of life, the child will grow by 12-13 cm, in the third - 7-8 cm.
Body mass.
In contrast to growth, body weight is a rather labile indicator, which reacts relatively quickly and changes under the influence of various reasons. Especially intense increase in body weight occurs in the first quarter of the year. The body weight of full-term newborns ranges from 2600g to 4000g and is on average 3-3.5 kg. However, adaptive body weight is 3250-3650 grams. Normally, for most children by the 3-5th day of life, there is a “physiological” decline in the mass of up to 5%. This is due to the greater loss of water with an insufficient amount of milk. Restoration of physiological weight loss occurs a maximum of 2 weeks.
The dynamics of body weight is characterized by a greater increase in the first 6 months of life and a lesser by the end of the first year. By 4.5 months, the body weight of a child doubles, triples by the year, despite the fact that this indicator may vary and depends on nutrition, past diseases, etc. The energy of increase in body weight with each month of life gradually decreases.
To determine the body weight at the age of one year is better to use the table. 3
Based on this table, the weight gain of the child for each subsequent month of life can be calculated by subtracting 50 grams from the previous month's increase (but only after the 3rd month), or by the formula: X = 800-50 x n, where 50 is a child increases in body weight 50 g less for each subsequent month of life, after the 3rd month; n is the number of months of a child's life minus three.
For example, in the tenth month of life a child adds a mass of 800- (50x7) = 450g.
There is another opinion that the average monthly weight gain in the first half of life is 800g, in the second half - 400g. However, it should be emphasized that the calculation according to the data given in table. 3 is considered preferable (physiological). Data on the assessment of body weight relative to height (body length) for boys and girls in centile intervals are given in Table. 4 and 5.
On average, by one year the child’s body weight is 10-10.5 kg. The increase in body weight in infants is not always characterized by such a pattern. It depends on the individual features child and a variety of external factors. Children with an initial low body mass give relatively large monthly weight gains and it doubles and triples earlier than in larger children. Babies who are bottle-fed immediately after birth, double their body weight about a month later than babies who are breast-fed. Body weight is a labile indicator, especially in a young child, and may change under the influence of various conditions sometimes during the day. Therefore, body weight is an indicator of the current state of the body, in contrast to growth, which does not immediately change under the influence of various conditions and is a more constant and stable indicator. The deviation of body weight from the norm to 10% is not considered pathology, however, the pediatrician should analyze this loss.
Proportionality of development.
In assessing the physical development of the child, it is necessary to know the correct relationship between body weight and height. The mass-mass index (MCI) is understood as the ratio of mass to height, i.e. what is the weight per 1 cm. of body length. Normal in newborns (MCI) is 60-75 g.
In addition to height and body weight, the correct proportions of the body matter to assess physical development. It is known that the chest circumference in full-term is less than the head circumference at birth. Head circumference in full-term infants varies widely enough - from 33.5 to 37.5 cm., On average equal to 35 cm. When analyzing these digital indicators, one should take into account the height and weight of the child, as well as the ratio of the head circumference to the chest circumference . When comparing it is necessary to take into account that at birth the head should not exceed the circumference of the chest by more than 2 cm. In the future it is necessary to focus on the growth rate of the circumference of the head. In the first 3–5 months, the monthly increase is 1.0–1.5 cm, and then 0.5–0.7 cm. By the year, the head circumference increases by 10–12 cm and reaches 46–47–48 cm (on average 47 cm.).
A child born with adaptive growth and body mass index has a head circumference of about 36 cm. In the first 3 months of life, the head circumference should “grow” by 4 cm (ie, in 3 months - 40 cm). Over the next 3 months, the head circumference increases by 3 cm and becomes 43 cm by 6 months, and by the year 46-48 cm. The dimensions of the large spring of the spring at birth should not exceed 2.5 x 3 cm, 3 x 3 cm.
The head circumference is measured at the position of a tape measure at the back at the level of the occiput, and in front at the eyebrows.
To characterize the physical development of the child is of great importance the correct assessment of the features of his chest, as the vital activity internal organs depends largely on the shape and size of the latter. The increase in the circumference of the chest most intensely occurs in the first year of life, especially in the first 6 months.
In a newborn, the chest circumference is 33-35 cm. The monthly increase in the first year of life is on average 1.5-2 cm. Per month. By the year, the chest circumference increases by 15-20 cm, after which the growth energy decreases and the chest circumference increases on average to preschool age 3 cm, and in pre-school - 1-2 cm per year.
For an individual assessment of the physical development of the child, it is important to know the periods of intersection of the circumference of the head and chest. In healthy children, this reversal occurs at about 3-4 months, and children who have at 5-7 months. there was no crossing, you need to take into account and analyze the dynamics of the development of the chest and head. An earlier reversal may indicate developing microcephaly, so it is necessary to monitor the timing of the closure of a large spring. The big spring should grow by the end of the first year in 80% of children, in the rest of children - by 1.5 years. The anterior-posterior size of the chest in most full-term newborns is less than or equal to the transverse diameter. Already during the first year of life, the transverse diameter begins to prevail over the anterior-posterior one and the shape of the chest flattens.
Statistical functions.
Static functions are estimated based on the rate of motor development of the child. These are the various motor skills of the child. It is necessary to take into account the ability of a child at a certain age to hold his head, make movements with his hands (feeling an object, grabbing, holding a toy in one hand, performing various actions), the appearance of dynamic functions (turning from back to stomach and from abdomen to back, pulling up, crawling, sitting down) , get up on your feet, walk, run).
At 2 months, the baby holds the head well,
at 3 months - turns well from back to stomach,
in 5.5 -6 months - it turns well from the abdomen to the back,
at 6 months - sitting, if he was put,
at 7.5 months, (when the child learns to crawl well) - he will sit himself,
at 9 months - well worth it,
in 10 months - walking around the arena, holding his hand,
by 12 months - walks alone.
The development of static functions contribute to the various exercises for children: from 1 to 3 months; from 3 to 6 months; from 6 to 9 months; from 9 to 12 months.
Timely eruption of milk teeth.
The teeth are laid about the 40th day of embryonic life. The child is born, as a rule, without teeth. Teething is a physiological act, the first teeth erupt at the age of 6 months. First, 2 lower middle incisors appear, by 8 months, 2 upper middle incisors appear, by 10 months, 2 upper lateral incisors appear. By the year 2 lateral lower incisors erupt. Thus, in 1 year of life a child should have 8 teeth - 4/4. By the age of 2, the eruption of the remaining 12 milk teeth ends. The bone system and the musculo-ligamentous apparatus in children, especially young children, are distinguished by their physiological weakness and require a strict dosed exercise.
Each of the indicators used, having an independent value, cannot serve as a criterion for the overall development of the child, if it is considered in isolation, and not in connection with other signs. Sex differences and indicators of physical development in the first year of life are expressed slightly.
Thus, physical development of a person is understood as a combination of morphological and functional features in their interrelation and interdependence on environmental conditions and hereditary factors.
4. Signs of the term of the newborn
The average body weight of a full-term newborn is 3,400 - 3,500 g for boys and 3,200 - 3,400 g for girls, while the fluctuations are very significant, but the lower limit of body weight for a full-term baby is 2,500.
The average body length is 50 cm, ranging from 48 to 52 cm. The mass and body length of children of multiparous mothers are usually greater than children of primiparas. The weight and height of children are influenced by the age of the parents, their state of health, the diet and the regimen of the woman during pregnancy.
The head circumference (32--33 cm) of a newborn is 2--4 cm longer than the chest, the length of the upper and lower extremities is the same, the chest circumference is 3--5 cm more than the half-growth, the thigh circumference is 2--3 cm less than the shoulder circumference . The umbilical ring is located midway between the womb and the xiphoid process.
The front part of the skull of a newborn is relatively small compared to the brain part. Most children have a well-defined scalp. On the head of the child after birth, there may be a generic tumor, which is formed as a result of the soft tissue being soaked with serous fluid. Its resorption occurs in the coming hours after birth, and rarely - on the 2nd - 3rd day. In the first hours after birth, the face of the newborn is somewhat swollen, the eyes are closed or half-open, the eyelids are somewhat swollen, the skin is pink, the subcutaneous fatty tissue is well developed.
The skin of the newborn is covered with the so-called original cheese-like lubricant, the amount of which varies considerably. On the shoulders and back, the skin is covered with a soft down.
The chest of the newborn is convex, short, inactive. The limbs are short, the legs are slightly convex anteriorly and outwards, therefore they appear to be curved. The muscles are underdeveloped, especially the muscles of the limbs. For newborns, pronounced hypertension of the muscles is characteristic, especially of the flexor limbs. The movements of the upper and lower limbs are irregular. The voice is loud, persistent cry. Unconditioned reflexes (sucking, swallowing, sneezing, coughing, etc.) are quite well expressed. In boys, the testicles are descended into the scrotum, in girls, the small lips and clitoris are covered with large labia.
For a more accurate characterization of the condition of the newborn, the Apgar scale is currently used, making an assessment within the 1st minute after the birth of the child.
5. Apgar Scale
The test was proposed by anesthesiologist Virginia Apgar.
Virginia Ampgar (born Virginia Apgar; June 7, 1909 - August 7, 1974) is an American anesthetist in obstetrics. The author of the famous Apgar scale. Born June 7, 1909 in Westfield, New Jersey (USA) in the family of Helen Clark and Charles Emory Apgar. In 1929 she graduated from Mount Holyoke College, in 1933- Columbia University College of Physicians & Surgeons. In the same place in 1937 she graduated from the residency in surgery. After that, she studied anesthesiology and in 1938 returned to Columbia University as head of the anesthesiology department. In 1949, Apgar became the first female professor at Columbia P & S, while at the same time she was engaged in research and research work at Sloane Hospital for Women. In 1959, she received her Master of Public Health degree from Johns Hopkins University. In 1953, proposed a test for assessing the health of newborns, the so-called. Apgar scale.
The result, recorded a minute after birth and recorded again after 5 minutes, reflects the general condition of the newborn and is based on observations in five assessment categories. The condition of children who score from 7 to 10 points is considered good or excellent, and they usually need only ordinary care; those who scored from 4 to 6 points are in a satisfactory condition, and they may need only some resuscitation procedures; and those whose outcome is less than 4 require immediate assistance to save their lives. At one time it was believed that children, whose result after 5 minutes after birth remained low, are doomed in the future to have neurological problems, but recent studies have shown that most of these children grow up normal and completely healthy.
The assessment consists of the sum of the numerical indicators of five signs. With the 8--10 indicator, the condition of the newborn is assessed as good, with the 6--7 indicator - satisfactory, and below 6 - heavy. For example, in a newborn, the heart rate is 120 per minute (grade 2), irregular breathing movements (1), the limbs are somewhat bent (1), the response to a nasal catheter is a grimace (1), the skin color is pink, limbs bluish (1); The Apgar score is 6.
Assessment of the condition of the newborn on the Apgar scale is almost completely acceptable, although it does not always reflect the diversity of possible disorders, especially in preterm.
6. Premature baby
A premature baby is a baby born with a period of less than 37 full weeks, i.e. up to 260 days of gestation.
The degree of prematurity:
degree 35-37 weeks weight approximately 2001--2500 g
degree 32-34 weeks weight approximately 1501--2000 g
degree 29-31 weeks weight approximately 1001--1500 g
degree less than 29 weeks weight less than 1000 g
What is the difference between premature babies and those born on time?
Nature knowingly invented that 9-month gestation in humans. At this time, the baby is formed and developed so that at the time of birth to be ready for extrauterine life. If for some reason a baby is born prematurely, it will be more difficult for him to adapt to the unknown and complex life outside of my mother's tummy. Of course, much depends on how earlier baby not full term If the birth occurred at 35-36 weeks, then the baby is already quite ripe, and if at 28-30 weeks, then it will take much more effort to care for it.
Premature babies usually have a disproportionate physique with short lower limbs and neck. The head looks larger in relation to the torso. The skin of a premature baby is thinner and delicate, covered with soft downy hair. Auricles are very soft. The subcutaneous fat layer in premature infants is not sufficiently formed, and even the fatty lumps on the cheeks are mild. All these signs can have a different degree of manifestation depending on the period of birth of the baby.
But not only external signs allow to distinguish a premature baby. The most important feature is the functional immaturity of all organs and systems of a premature newborn. So, premature babies retain heat worse, they are more sluggish and drowsy, they are characterized by a decrease in muscle tone and sluggish sucking. Of course, these functional features are more pronounced, the smaller the child.
What is nursing premature?
After birth, a premature baby requires special attention from doctors. Regardless of the degree of maturity and prematurity, the child must be given first aid - to warm, suck the amniotic fluid from the mouth, provide additional oxygen, and in more severe cases - to carry out a full range of resuscitation.
The severity of the condition of the premature baby may be due to several reasons. First of all, pediatricians pay attention to the formation of respiratory function. In the lungs of a premature baby, there is not enough special substance produced - surfactant, which helps them to fully function: it prevents the alveoli from falling and ensures normal gas exchange. A lack of surfactant can cause various respiratory disorders — from mild respiratory distress syndrome to severe illness, in which spontaneous breathing is impossible and artificial lung ventilation is required.
Respiratory failure exacerbates existing metabolic changes in the child caused by birth stress, and problems with the circulatory system, digestion, discharge.
To create a comfortable thermal regime for a premature baby, the baby is placed in a incubator. In parallel with this, correction of all existing violations is carried out. After the premature baby begins to retain heat better, is able to breathe independently, and he does not need intensive therapy, he can be transferred from the maternity hospital to the second stage of nursing in a specialized department for premature babies. If premature birth occurred in a specialized maternity hospital, then such a unit is well included in its composition. Such a unit may be part of a maternity hospital, if the hospital specializes in preterm labor, or at a children's hospital.
Nursing a premature baby at this stage is a logical continuation of the activities initiated in the wards of the maternity hospital. The period of adaptation to extrauterine life in a premature baby also has some differences compared to a full-term baby. So, weight loss in premature babies is usually greater than in babies born on time. Recovery of the initial body weight occurs over a longer period: full-term babies usually recover their weight at birth by the age of 7–10, and for premature babies, this period can last for 2–3 weeks.
Another condition that occurs in newborns is physiological jaundice. But in premature babies jaundice is more pronounced and its duration is longer than in term babies, which in some cases requires treatment. This is due to the functional features and immaturity of liver enzymes. Feeding a premature baby can also cause some problems, since premature babies do not digest well. Feed infants begin to literally drop by drop, gradually increasing the volume. Optimal for premature babies is breastfeeding mothers. As is known, the composition of the milk of a woman who gave birth prematurely differs from the milk of the mother, whose birth occurred on time. It contains more protein, electrolytes, polyunsaturated fatty acids, and less lactose, better serving the needs of a small baby. In the event that breastfeeding is not possible, the child should receive a specialized mixture for premature babies.
When is a premature baby being discharged home?
This question worries many many parents whose babies were born prematurely. Of course, such decisions are made by doctors, based on the state of the child. Usually, if the child’s weight reaches 2000 g, the baby is actively sucking and gaining weight, it can be discharged under the condition of active supervision at home by the pediatrician and the nursing nurse. In addition, after discharge from the hospital, the baby may need additional help from an oculist, neurologist, massage therapist and some other specialists.
In conclusion, you need to add that a baby born prematurely needs not only experienced and competent doctors and nurses, but also the love and care of mom and dad. Nursing premature is a time consuming and long process. But a premature baby has every chance to catch up with its peers over time, and in the future not to differ from them in mental and motor development.
A premature baby requires close attention, as there are often a number of problems in the process of nursing. First of all, this applies to children born with a weight of 1,500 g and less “very premature” and, especially, less than 1,000 g “extremely premature”. It should be remembered that the division into degrees of prematurity, taking into account the weight parameters, does not always correspond to the true conceptual age of the child. This classification method is used to standardize treatment and observation, for the needs of statistics. In practice, in addition, it is necessary to take into account a wider range of positions to assess the actual age of the child.
The frequency of preterm birth is variable, but in most developed countries in recent decades is quite stable and amounts to 5-10% of the number of children born. The reasons for under-wearing can be divided into three large groups:
Socio-economic and demographic. Lack or insufficiency of medical care, poor nutrition of a pregnant woman, occupational hazards (work on the conveyor, physical activity, standing for most of the working day), bad habits, unwanted pregnancy, etc.
Socio-biological. Preterm birth is more common in primiparous women under the age of 18 and over 30 years of age; the father’s age is over 50 years old. The obstetric history is important: artificial interruption of pregnancy (especially criminal or proceeding with complications), pregnancy that occurred shortly after giving birth (less than 2-3 years).
Clinical. The presence of pregnant somatic, gynecological, endocrinological diseases. Pathology of pregnancy: late preeclampsia, acute infectious diseases, transferred during pregnancy, surgery, physical injuries especially of the abdomen.
Pathology of the newborn: intrauterine infections, malformations, chromosomal abnormalities. The survival rate of premature babies depends directly on the gestational age and body weight at birth. The group of children weighing less than 1500 g and below (less than 30-31 weeks of gestation) is less than 1% of live births, but 70% of deaths of newborns. During the shortened period of stay in the mother’s womb, premature babies didn’t have enough time to prepare for extra-uterine conditions, they didn’t accumulate enough nutrients.
The group of low-weight children especially depends on the influence of external factors. They require ideal nursing conditions in order to achieve not only their survival, but also favorable further development.
One of the most important conditions for nursing premature babies is the optimum temperature immediately after the birth of the child is placed in an environment with air temperature from 34 to 35.5 degrees (the lower the child’s weight the higher the temperature) by the end of the month the temperature is gradually reduced to 32 degrees.
Another important condition for nursing is humidity and in the first days it should be 70-80%.
These conditions are observed when a child is placed in a cooler (incubator for nursing newborns), where children weighing up to 1500 g are usually placed. Also, the thermal regime can be maintained using special changing tables with a source of radiant heat.
Special mention should be made about feeding premature babies. Babies born before 33-34 weeks of gestation, as a rule, are fed through a tube inserted into the stomach every 3 hours.
7. Anatomical and physiological features of a premature baby
Premature babies have a peculiar physique - a relatively large head with a predominance of the cranial skull, sometimes - open cranial sutures, small and lateral fontanelles, low position of the umbilical ring; poor development of subcutaneous fat. Abundant hair growth (lanugo) is typical for premature babies, with a significant degree of prematurity - underdevelopment of the nails. The bones of the skull are malleable due to insufficient mineralization; the auricles are soft. In boys, the testicles are not descended into the scrotum (in extremely immature children, the scrotum is generally underdeveloped); in girls, the genital gap gapes due to underdevelopment of the labia majora and relative clitoral hypertrophy. On the basis of an external examination of the child, it is possible to make a conclusion about the degree of prematurity (gestational age) on the basis of a set of morphological criteria, for which purpose evaluation tables of these signs in points have been developed.
The nervous system of premature babies is characterized by weakness and rapid extinction of physiological reflexes (in very premature babies, including sucking and swallowing); delayed reaction to irritation; imperfect thermoregulation; muscle hypotonia.
The morphology of the brain of a premature baby is characterized by smoothness of the grooves, weak differentiation of gray and white matter, incomplete myelination of nerve fibers and pathways.
The reactions of premature babies to various stimuli are distinguished by generalization, weakness of active inhibition, and irradiation of the arousal process. The immaturity of the cortex causes the predominance of subcortical activity: movements are chaotic, there can be marked flinches, hand tremors, clonus of the feet.
Due to the immaturity of the thermoregulatory mechanisms, premature babies cool easily (reduced heat production and increased heat transfer), they do not have an adequate increase in body temperature during the infectious process and they easily overheat in incubators. Overheating contributes to the underdevelopment of sweat glands.
The system of respiratory organs in a premature baby, as well as the nervous system, is characterized by immaturity (a predisposing background for pathology). The upper respiratory tract in prematurely narrow, the diaphragm is relatively high, the chest is supple, the ribs are perpendicular to the sternum, in the very premature babies the sternum sinks. Breathing is superficial, weakened, the frequency of 40--54 per minute, the volume of breathing as compared with full-term children is reduced. Respiratory rhythm irregular, with periodic apnea.
The cardiovascular system of a premature baby in comparison with other functional systems is relatively mature, as it is laid in the early stages of ontogenesis. Despite this, the pulse in premature babies is very labile, of weak filling, the frequency is 120-160 per minute. For the most immature children, the rhythmic pattern of the embryocardia type is characteristic. Auscultation heart sounds may be relatively muffled; with the persistence of embryonic shunts (canal duct, oval window), noise may be present. Blood pressure in premature infants compared with full-term lower: systolic 50--80 mm Hg. Art., diastolic 20--30 mm Hg. Art. The average pressure of 55--65 mm Hg, Art.
In connection with the increased load on the right parts of the heart, electrocardiograms of premature are characterized by signs of the grammar card and a high P wave combined with relatively low voltage and smoothness of the S interval. T.
The gastrointestinal tract of premature babies is characterized by the immaturity of all departments, a small volume and a more upright position of the stomach. Due to the relative underdevelopment of the cardiac muscles, premature babies are prone to regurgitation. The mucous membrane of the digestive canal in premature babies is tender, thin, easily vulnerable, richly vascularized. There are low protheolytic activity of gastric juice, insufficient production of pancreatic and intestinal enzymes, as well as bile acids. All this complicates the processes of digestion and absorption, contributes to the development of flatulence and dysbacteriosis. Two-thirds of premature babies, even while breastfed, have a deficiency in intestinal bifidoflora combined with carriage of conditionally pathogenic flora. The nature of the child’s stool is determined by the feeding characteristics; As a rule, in coprogram frame in prematurely, a lot of neutral fat.
Features of the functioning of the endocrine system of a premature baby are determined by the degree of its maturity and the presence of endocrine disorders in the mother, which caused preterm birth. As a rule, the coordination of the activity of the endocrine glands is disturbed, primarily along the axis of the pituitary gland - the thyroid gland - the adrenal glands. The process of the reverse development of the fetal zone of the adrenal cortex in newborns is inhibited, the formation of circadian rhythms of hormone release is delayed. Functional and morphological immaturity of the adrenal glands contributes to their rapid depletion.
In premature infants, the reserve capacity of the thyroid gland is relatively reduced, and therefore they may develop transient hypothyroidism. The sex glands in premature babies are less active than in full-term babies, which is why their so-called sexual crisis in the first days of life is much less common.
The processes of metabolic adaptation in premature babies are slow. At the age of 4--5 days, they more often have metabolic acidosis in the blood plasma in combination with a compensatory shift towards alkalosis inside the cell; in the 2--3rd week of life, extracellular acidosis is compensated by intracellular normidirectional reactions. In premature babies (even conditionally healthy), hypoglycemia, hypoxemia, and hyperbilirubinemia are more common.
The renal regulation of the acid-base state and electrolyte composition in premature babies is not perfect; water-salt metabolism is labile, which is both a tendency to the occurrence of edema and rapid dehydration in pathologically states or inadequate care. The immaturity of the kidney causes a relatively high rate of residual nitrogen in the blood of premature babies in the first 3 days of life (up to 34.4 mmol / l), in the following days this figure decreases; in premature babies, a relatively stable diuresis is established. Urine is weakly concentrated (due to the low concentration ability of the kidneys), the frequency of urination usually exceeds that of the full-term (relatively high intensity of metabolism and water-food load).
8. Anatomical and physiological features of full-term children
Leather. Gentle, velvety to the touch, elastic, pink, there may be remnants of fluffy hair on the back and shoulder girdle. Its richness in blood vessels and capillaries, poor development of the sweat glands and vigorous sebaceous activity leads to a rapid overheating or overcooling of the child. He has easily vulnerable skin, which is also important to consider, because with improper care, diaper rash appears, infection easily penetrates through the pores and pustules appear. On the occiput, upper eyelids, between the eyebrows there may be bluish or reddish spots, caused by the expansion of blood vessels (telangiectasia), or pinpoint hemorrhages. Sometimes there are yellowish-white nodules (milia) on the wings and back of the nose. All these phenomena disappear in the first months of life. In the area of the sacrum, there may also be an accumulation of skin pigment, the so-called. "Mongolian spot". It remains noticeable for a long time, sometimes for the whole life, however, it is not a sign of any violations. The hair of a newborn up to 2 cm in length, eyebrows and eyelashes are almost imperceptible, nails reach to the tips of the fingers.
Subcutaneous fat. Well developed, more dense than it will become in the future - by its chemical composition, it is now dominated by refractory fatty acids.
Bone system. It contains little salt, giving it strength, so the bones easily bend when improperly caring for a child.
The infant feature is the presence of non-ossified areas in the skull - the so-called. springs Large, in the form of a rhombus, located in the region of the junction of the parietal and frontal bones, size 1.8-2.6 x 2-3 cm. Small, in the form of a triangle, located at the convergence of the parietal and occipital bones, and in most children at birth is closed . Such a soft connection of the bones of the skull is of practical importance when the head passes through the narrow birth canal. Its regular deformation into an elongated "pear" is not terrible and should not cause a "panic". Correct shape is a matter of time. Should not frighten parents and striking disparity of body parts of the baby. Indeed, the head looks too large, because 1-2 cm more circumference of the chest, arms are much longer than the legs. The existing disproportion is also a matter of time, which will fix everything.
The chest is barrel-shaped: the ribs are arranged horizontally, not obliquely, as in the future. They consist mainly of cartilage, as well as the spine, which does not yet have physiological curves. They will form later, when the child begins to sit and stand.
Muscular system. Their increased tone prevails - the arms are bent at the elbows, the legs are pressed to the abdomen: the uterine posture according to the remaining inertia. The neck does not hold the head - its muscles are weak. The child “twins” her arms and legs continuously, but targeted movements and motor skills will come with the maturity of the nervous system.
Respiratory system. The mucous membranes of the respiratory tract are tender, contain a greater number of blood vessels, therefore, with infections, often viral, swelling quickly develops, a large amount of mucus is secreted, which makes breathing difficult. It is also obstructed by the anatomical narrowness of the nasal passages of the newborn, as well as his trachea (respiratory throat) and bronchi. The auditory or Eustachian tube is wider and shorter than in older children, which facilitates infection and otitis media (inflammation of the middle ear). But then there is never inflammation of the frontal sinus (frontal sinus) and maxillary, or maxillary, sinuses (antritis), since they are still missing. The lungs are underdeveloped, breathing is shallow and is mainly carried out by the diaphragm, a muscle located on the border of the chest and abdominal cavities. Therefore, breathing is easily disturbed by the accumulation of gases in the stomach and intestines, constipation, tight swaddling, pushing the diaphragm up. Hence the desire - to monitor the regular emptying of the intestines, do not swaddle the child too tight. Since the infant does not receive enough oxygen in its shallow breathing, it breathes often. Norm 40-60 breaths per minute, but this frequency increases even with a slight load. Therefore, it is necessary to pay attention primarily to shortness of breath, which is accompanied by a feeling of lack of air and can be a sign of the disease.
The cardiovascular system. With the birth of a newborn, changes in the circulatory system occur, at first functional - the umbilical vessels and vein cease their activity, and then anatomical - the intrauterine channels of the blood flow are closed. With the first inhalation, the small circle of blood circulation comes into operation, passing through which the blood is saturated with oxygen in the lung tissue. Heart rate 120-140 beats per minute, when feeding or crying increases to 160-200 beats. Blood pressure at the beginning of the first month 66/36 mm Hg. Art., and by the end of it - 80/45 mm Hg. Art.
Introduction Healthy child
"... and that's when they asked to bring the most beautiful thing in the whole wide world, the crow brought her child ..."
The first fragmentary information about a healthy and sick child appeared in ancient times. Hippocrates, Galen, Soran, Avicenna emphasized in their treatises the presence of features of a children's organism that distinguishes it from an adult and determines the atypical course of diseases, especially in early childhood. Even then, scientists paid much attention to the importance of breastfeeding, physical education and proper care for the harmonious growth and development of the child.
Russian scientists have made a huge contribution to the development of national pediatrics. N.F. Filatov - the founder of domestic pediatrics, N.P. Gundobin, the author of the classification of periods of childhood, and other scholars, in their works, singled out sections on healthy children, feeding and upbringing.
In the modern world, time needs to be given great attention to the development and upbringing of children, since children are the future of our planet.
1. Periods of childhood
The body of the child all the time is in the process of growth and development, which occur continuously in a certain regular sequence. From the moment of birth to an adult, a child goes through certain age periods.
A child in different periods of life is characterized by certain anatomical and physiological features, the totality of which affects the reactive properties and body resistance. This explains the peculiarity of the pathology, and the peculiar course of certain diseases in children of different age groups.
But we should not think that the age characteristics of the child themselves doomed him to the disease. If the environmental conditions, temperature, nutrition, care, use of fresh air, etc. meet the requirements of the body of a newborn or infant, then this creates the prerequisites for its proper growth, development and protection from diseases. Conversely, adverse environmental conditions adversely affect the health of the child. Even small errors in care, nutrition, and temperature can adversely affect the health of a child, especially a newborn and an infant.
The most acceptable for practical purposes is the N. N. Gundobin scheme, according to which the entire childhood age is divided into the following periods.
Gundobin Nikolay Petrovich, Russian pediatrician. He graduated in 1885, medical faculty of Moscow University. Since 1897 Professor of the Department of Children's Diseases of the Military Medical Academy in St. Petersburg. The main works are devoted to the study of the age characteristics of the anatomy, physiology and pathology of the children's body. Gundobin N.P. He was chairman of the school department of the Society for the Conservation of Public Health and one of the organizers (1904, together with N. A. Russkikh) of the Union to Combat Child Mortality.
Cit .: The education and treatment of a child up to the age of seven, 3rd ed., M., 1913; Features of childhood, St. Petersburg, 1906.
I. The period of prenatal development: 1) the phase of embryonic development (embryo), 2) the phase of placental development (fetus).
Ii. The neonatal period.
Iii. The period of infancy (younger nursery),
Iv. The period of milk teeth: a - preschool age (older nursery), b - preschool age (period of attendance at kindergarten).
V. The period of adolescence (primary school age).
Vi. Puberty (senior school age).
In parentheses are marked all the changes that have been made by Soviet pediatricians.
This division is conditional, and it is rather difficult to draw clear lines between periods. But they are convenient to use when studying the physiological and pathological conditions of the child, as well as for practical therapeutic and preventive purposes.
2. Stages of intrauterine development
In prenatal human development, there are conventionally three periods:
The implantation period lasts from the moment of fertilization to 2 weeks. This period is characterized by rapid systematic fragmentation of a fertilized egg, its promotion through the fallopian tube to the uterus; implantation (embryo attachment and implantation into the uterine mucosa) on days 6–7 after fertilization and further formation of the membranes, creating the necessary conditions for the development of the embryo. They provide nutrition (trophoblast), create a liquid habitat and mechanical protection (fluid of the fetal bladder).
The embryonic period lasts from the 3rd to the 10th – 12th week of pregnancy. During this period, the rudiments of all the most important organs and systems of the future baby are formed, the body, head and limbs are formed. The placenta is developing - the most important organ of pregnancy, which separates the two blood flows (mother and fetus) and ensures the exchange of substances between the mother and the fetus, protecting it from infectious and other harmful factors, from the mother’s immune system. At the end of this period, the embryo becomes a fetus that has a childlike configuration.
The fetal period begins with the 3rd month of pregnancy and ends with the birth of a child. Nutrition and metabolism of the fetus through the placenta. There is a rapid growth of the fetus, the formation of tissues, the development of organs and systems from their buds, the formation and formation of new functional systems that ensure the life of the fetus in the womb of the mother and child after birth.
After the 28th week of pregnancy, the fetus begins to form a reserve of valuable substances needed during the first time after birth - salts of calcium, iron, copper, vitamin B12, and others. Maturation of the surfactant, which provides normal lung function, occurs. Fetal development is affected by various environmental factors. They have the most significant effect on the organs that develop most intensively at the time of exposure.
3. Thoracic period
The chest period, from 4 weeks to 1 year of life, is characterized by an intense increase in body weight and growth, by intense physical, psychological and intellectual development. By 4 months, body weight doubles, and by 1 year - tripled.
For the first quarter of the year, the child grows monthly by 3 cm, for the second quarter - by 2.5 cm, for the third quarter - by 1.5 cm and for the fourth quarter of the year, the child each month adds 1 cm to his height. in the psychomotor development of the child, during this period the foundation of health, physical and mental development is laid. It is estimated every quarter of the year.
In the development of the visual analyzer, the following occurs: by the end of the 1st month, visual concentration is observed; k 2 - 3 rd month - fixing the gaze with simultaneous reactions of the muscles of the neck and head; by 3.5 months - distinguishing surrounding objects, prolonged concentration, tracking of objects; by 5 months, the ability to view an object at close range is manifested; for 6 months, the child clearly distinguishes colors, expressing a definite relationship to them.
Reactions of the auditory perception are manifested, in addition to auditory concentration (end of the 2nd week), a clear orientation to the sounds (1st month) and the search for its source from the end of the 2nd month. At 2–3 months, the child listens to sounds, and at 3–3.5 months, he unmistakably searches for the sound source. In 3–7 months, there is a constant activity on various sound stimuli, and from 10–11 months there is a reaction to the sound in connection with the content and meaning of this sound.
The development of the child’s motor skills - keeps the head upright if it is held upright (at the 5th – 6th week), lifts the head or turns it to the side in a position on the stomach (at the 5th week), turns over on its side from the position lying on its back (4–4.5 months), sits independently (6–7 months), walks on all fours (at the 8th month), rises and stands, adhering to the support (7–8 months), walks independently (at 11–12 m month).
Development of grasping ability - stretches a hand to the object (at the 3rd month), seizes the object (4.5 months), holds the object in each hand (6 months), brings the whole body to the active state when grabbing (at the 7th month ), the beginnings of specific manipulations (on the 11th month).
Teething from 5-7 months.
From 4–6 weeks, visual-auditory search and visual concentration on the adult’s face are observed, and from 3 months there is a pronounced need for communication with adults. In an infant, the leading line of physical activity at 7–8 months is crawling; in the 12th month, the rudiments of manipulation games.
The development of the I and II signaling systems of the central nervous system, the thymus and thyroid glands are functioning; adrenal function weakened; start of pituitary function.
Rachitis, dystrophy, food and respiratory allergies, respiratory diseases and acute gastrointestinal diseases can occur.
In each period for the proper development of the child requires the creation of certain environmental conditions, regime, education.
Features of growth and development
Significant growth rates are characteristic - body length (growth) increases by 50% at birth, reaches 75–77 cm by 1 year. Head circumference is 46–47 cm by year, breast circumference is 48 cm. Motility and motor skills are developing rapidly. . Three peaks of motor activity are distinguished: I - 3-4 months - a complex of revival, joy at the first contact with adults; II - 7-8 months - crawling activation, formation of binocular vision (mastering the space); III peak - 11-12 months - the beginning of the walk. Their sensory-motor connections are determined. Skeletal muscles and physical activity are the factors determining the processes of growth and development in the first year of a child's life. The growth rate is ensured by a high metabolism.
Features of the central nervous system
An increase in the brain mass by one year is 2-2.5 times, the most intensive differentiation of nerve cells in the first 5-6 months of life. Not enough activity-aminobutyric acid (inhibitory factor) and little myelin, which contributes to the rapid spread of any excitement.
An approximate reflex is maintained, reflecting the innate need for movement and the activity of the sense organs. Nervous connections between the child and surrounding people are established through facial expressions, gestures, and voice intonations. The development of subtle hand movements contributes to the development of brain and speech. There are connections between words and motor response reactions of the child, then the child connects the visual and auditory perception of objects with the words, the names of the objects when they are shown, and links with individual actions (“give”, “show”) - this is the optimal course of development necessary as a basis for other periods of childhood. The need for contact with adults determines the mental development of the child.
Electroencephalogram in 2-3 months - steady rhythm; in 4-6 months - changes are unidirectional; in 8-10 months - progressive individualization.
Features of the endocrine system
In the thoracic period, there is an increase in the function of the pituitary and thyroid glands. They stimulate the growth and development of the child, metabolism, provide normal differentiation of the brain and intellectual development. Adrenal function is enhanced, partial involution of the adrenal fetal cortex occurs, and the biological activity of corticosteroids is increased.
Immunity Features
There is a slight decrease in the number of T and B cells in the blood compared with the neonatal period. A decrease in maternal IgG from 2–3 months was expressed, the synthesis of its own IgG increased from 2–3 months; its constant level is established after 8 months - 1 year. The level of IgM by the end of the year is 50% of the adult level. The concentration of IgA slowly increases. IgE in a healthy child is contained in insignificant amounts, its level depends on the manifestations of allergy (increases). The second critical period of immunity is noted at 4-6 months and is characterized by: the lowest level of specific antibodies - physiological hypogammaglobulinemia; synthesis of IgM antibodies that leave no immunological memory. An atypical flow of measles, whooping cough - leaving no immunity! High sensitivity to respiratory syncytial infection, parainfluenza viruses and adenoviruses remains.
Non-specific resistance factors
Typically high levels of lysozyme and properdin. By the end of the first month of life, the level of complement rapidly increases and reaches the level of an adult. From 2–6 months, the final phase of phagocytosis of leukocytes to pathogenic microorganisms, with the exception of pneumococcus, staphylococcus, Klebsiella, hemophilus bacilli, is formed.
Nature of pathology
Often develop respiratory diseases, acute gastrointestinal diseases, food allergies, rickets, degeneration, iron deficiency anemia. Possible manifestation of hereditary diseases, tuberculosis, syphilis, HIV infection.
Assessment of physical development, motor skills, speech development, neuropsychic development, taking into account the leading line of development in the thoracic period, is carried out quarterly.
To assess the physical development of children under 1 year old it is better to use the following indicators:
Body mass;
Proportionality of development (head circumference; chest circumference, some anthropometric indices);
Static functions (motor skills of the child);
Timely eruption of milk teeth (in children up to 2 years).
The skull of a newborn has specific features. See fig.
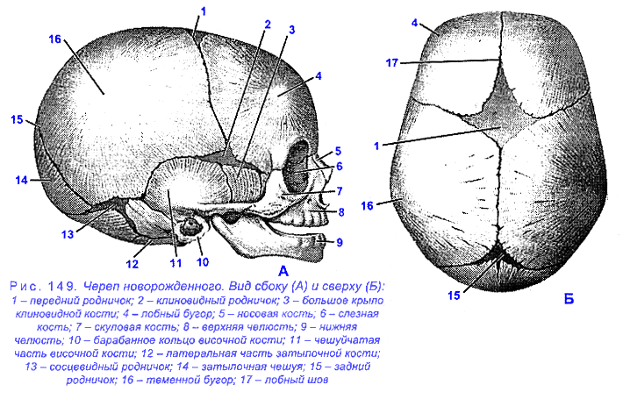
The most stable indicator of physical development is the growth of the child. It determines the absolute length of the body and, accordingly, the increase in body size, development, maturation of its organs and systems, the formation of functions in one or another period of time.
The highest growth energy is in the first quarter of the year (Table A). In full-term newborns, growth ranges from 46 to 60 cm. On average, 48-52 cm, but adaptive growth rates are considered to be 50-52 cm. This means that adaptation in the prenatal period occurred not only at the organism level, but also at the organ level and enzymatic.
Table A. Increase in height and body weight in children of the first year of life
| Age, months | Growth gain for the month, see | Growth over the past period, see | Monthly weight gain, gr. | The increase in body weight over the past period, gr. |
| 1 | 3 | 3 | 600 | 600 |
| 2 | 3 | 6 | 800 | 1400 |
| 3 | 2,5 | 8,5 | 800 | 2200 |
| 4 | 2,5 | 11 | 750 | 2950 |
| 5 | 2 | 13 | 700 | 3650 |
| 6 | 2 | 15 | 650 | 4300 |
| 7 | 2 | 17 | 600 | 4900 |
| 8 | 2 | 19 | 550 | 5450 |
| 9 | 1,5 | 20, 5 | 500 | 5950 |
| 10 | 1,5 | 22 | 450 | 6400 |
| 11 | 1,5 | 23, 5 | 400 | 6800 |
| 12 | 1,5 | 25 | 350 | 7150 |
During the first year, the child grows an average of 25 cm in height, so that by the year his height averages 75-76 cm. With the right development of the child, the monthly increase in growth can vary within ± 1 cm, but by 6 months and by the year these fluctuations height should not exceed 1 cm.
Growth reflects the characteristics of plastic processes occurring in the human body. Hence the importance of high-quality nutrition, especially the content of a sufficient amount of a balanced full-fledged protein component and vitamins of group B, as well as A, D, E. Certainly, the “gold standard” of optimal nutrition for children under 1 year old is breast milk. The deficiency of some food components selectively disrupts growth in children. These include vitamin A, zinc, iodine. Growth can be caused by various chronic diseases.
Growth measurements for a child in the first year of life are made on a horizontal stadiometer. Measurements are made by 2 people. Measuring is on the right side of the child. The helper keeps the child's head in a horizontal position so that the upper edge of the ear trestle and the lower edge of the orbit are in the same plane perpendicular to the height plate. The apical part of the head should touch the vertical fixed bar. The arms of the child are extended along the body. Measuring with a light pressure on the child's knees with his left hand, he holds his legs in a straightened position, and with his right hand pushes the moving bar of the height meter tightly to the plantar side of the feet, bent at a right angle.
For the second year of life, the child will grow 12-13 cm, for the third - 7-8 cm.
Body mass.
In contrast to growth, body weight is a rather labile indicator, which reacts relatively quickly and changes under the influence of various reasons. Especially intense increase in body weight occurs in the first quarter of the year. The body weight of full-term newborns ranges from 2600g to 4000g and is on average 3-3.5 kg. However, adaptive body weight is 3250-3650 grams. Normally, for most children by the 3-5th day of life, there is a “physiological” decline in the mass of up to 5%. This is due to the greater loss of water with an insufficient amount of milk. Restoration of physiological weight loss occurs a maximum of 2 weeks.
The dynamics of body weight is characterized by a greater increase in the first 6 months of life and a lesser by the end of the first year. By 4.5 months, the body weight of a child doubles, triples by the year, despite the fact that this indicator may vary and depends on nutrition, past diseases, etc. The energy of increase in body weight with each month of life gradually decreases.
To determine the body weight at the age of one year is better to use the table. 3
Based on this table, the weight gain of the child for each subsequent month of life can be calculated by subtracting 50 grams from the previous month's increase (but only after the 3rd month), or by the formula: X = 800-50 x n, where 50 is a child increases in body weight 50 g less for each subsequent month of life, after the 3rd month; n is the number of months of a child's life minus three.
For example, in the tenth month of life a child adds a mass of 800- (50x7) = 450g.
There is another opinion that the average monthly weight gain in the first half of life is 800g, in the second half - 400g. However, it should be emphasized that the calculation according to the data given in table. 3 is considered preferable (physiological). Data on the assessment of body weight relative to height (body length) for boys and girls in centile intervals are given in Table. 4 and 5.
On average, by one year the child’s body weight is 10-10.5 kg. The increase in body weight in infants is not always characterized by such a pattern. It depends on the individual characteristics of the child and a number of external factors. Children with an initial low body mass give relatively large monthly weight gains and it doubles and triples earlier than in larger children. Babies who are bottle-fed immediately after birth, double their body weight about a month later than babies who are breast-fed. Body weight is a labile indicator, especially in a young child, and may change under the influence of various conditions sometimes during the day. Therefore, body weight is an indicator of the current state of the body, in contrast to growth, which does not immediately change under the influence of various conditions and is a more constant and stable indicator. The deviation of body weight from the norm to 10% is not considered pathology, however, the pediatrician should analyze this loss.
Proportionality of development.
In assessing the physical development of the child, it is necessary to know the correct relationship between body weight and height. The mass-mass index (MCI) is understood as the ratio of mass to height, i.e. what is the weight per 1 cm. of body length. Normal in newborns (MCI) is 60-75 g.
In addition to height and body weight, the correct proportions of the body matter to assess physical development. It is known that the chest circumference in full-term is less than the head circumference at birth. Head circumference in full-term infants varies widely enough - from 33.5 to 37.5 cm., On average equal to 35 cm. When analyzing these digital indicators, one should take into account the height and weight of the child, as well as the ratio of the head circumference to the chest circumference . When comparing it is necessary to take into account that at birth the head should not exceed the circumference of the chest by more than 2 cm. In the future it is necessary to focus on the growth rate of the circumference of the head. In the first 3–5 months, the monthly increase is 1.0–1.5 cm, and then 0.5–0.7 cm. By the year, the head circumference increases by 10–12 cm and reaches 46–47–48 cm (on average 47 cm.).
A child born with adaptive growth and body mass index has a head circumference of about 36 cm. In the first 3 months of life, the head circumference should “grow” by 4 cm (ie, in 3 months - 40 cm). Over the next 3 months, the head circumference increases by 3 cm and becomes 43 cm by 6 months, and by the year 46-48 cm. The dimensions of the large spring of the spring at birth should not exceed 2.5 x 3 cm, 3 x 3 cm.
The head circumference is measured at the position of a tape measure at the back at the level of the occiput, and in front at the eyebrows.
To characterize the physical development of the child, the correct assessment of the features of his chest is of great importance, since the vital activity of the internal organs depends largely on the shape and size of the latter. The increase in the circumference of the chest most intensely occurs in the first year of life, especially in the first 6 months.
In a newborn, the chest circumference is 33-35 cm. The monthly increase in the first year of life is on average 1.5-2 cm. Per month. By the year, the chest circumference increases by 15-20 cm, after which the growth energy decreases and the chest circumference increases by an average by 3 cm by the pre-school age, and by 1-2 cm per year in the pre-school age.
For an individual assessment of the physical development of the child, it is important to know the periods of intersection of the circumference of the head and chest. In healthy children, this reversal occurs at about 3-4 months, and children who have at 5-7 months. there was no crossing, you need to take into account and analyze the dynamics of the development of the chest and head. An earlier reversal may indicate developing microcephaly, so it is necessary to monitor the timing of the closure of a large spring. The big spring should grow by the end of the first year in 80% of children, in the rest of children - by 1.5 years. The anterior-posterior size of the chest in most full-term newborns is less than or equal to the transverse diameter. Already during the first year of life, the transverse diameter begins to prevail over the anterior-posterior one and the shape of the chest flattens.
Statistical functions.
Static functions are estimated based on the rate of motor development of the child. These are the various motor skills of the child. It is necessary to take into account the ability of a child at a certain age to hold his head, make movements with his hands (feeling an object, grabbing, holding a toy in one hand, performing various actions), the appearance of dynamic functions (turning from back to stomach and from abdomen to back, pulling up, crawling, sitting down) , get up on your feet, walk, run).
At 2 months, the baby holds the head well,
at 3 months - turns well from back to stomach,
5.5–6 months - it turns well from the belly to the back,
at 6 months - sitting, if he was put,
at 7.5 months, (when the child learns to crawl well) - he will sit himself,
at 9 months - well worth it,
in 10 months - walking around the arena, holding his hand,
by 12 months - walks alone.
The development of static functions contribute to the various exercises for children: from 1 to 3 months; from 3 to 6 months; from 6 to 9 months; from 9 to 12 months.
Timely eruption of milk teeth.
The teeth are laid about the 40th day of embryonic life. The child is born, as a rule, without teeth. Teething is a physiological act, the first teeth erupt at the age of 6 months. First, 2 lower middle incisors appear, by 8 months, 2 upper middle incisors appear, by 10 months, 2 upper lateral incisors appear. By the year 2 lateral lower incisors erupt. Thus, in 1 year of life a child should have 8 teeth - 4/4. By the age of 2, the eruption of the remaining 12 milk teeth ends. The bone system and the musculo-ligamentous apparatus in children, especially young children, are distinguished by their physiological weakness and require a strict dosed exercise.
Each of the indicators used, having an independent value, cannot serve as a criterion for the overall development of the child, if it is considered in isolation, and not in connection with other signs. Sex differences and indicators of physical development in the first year of life are expressed slightly.
Thus, physical development of a person is understood as a combination of morphological and functional features in their interrelation and interdependence on environmental conditions and hereditary factors.
4. Signs of the term of the newborn
The average body weight of a full-term newborn is 3400-3500 g for boys and 3200-3400 g for girls, while the fluctuations are quite significant, but 2500 g is considered the lower limit of body weight for a full-term baby.
The average body length is 50 cm, ranging from 48 to 52 cm. The mass and body length of children of multiparous mothers are usually greater than children of primiparas. The weight and height of children are influenced by the age of the parents, their state of health, the diet and the regimen of the woman during pregnancy.
The circumference of the head (32-33 cm) of a newborn is 2–4 cm longer than the chest, the length of the upper and lower extremities is the same, the chest is 3-5 cm longer than the half-growth, the circumference of the hips is 2-3 cm less than the circumference of the shoulders. The umbilical ring is located midway between the womb and the xiphoid process.
The front part of the skull of a newborn is relatively small compared to the brain part. Most children have a well-defined scalp. On the head of the child after birth, there may be a generic tumor, which is formed as a result of the soft tissue being soaked with serous fluid. Its resorption occurs in the coming hours after birth and rarely on the 2-3rd day. In the first hours after birth, the face of the newborn is somewhat swollen, the eyes are closed or half-open, the eyelids are somewhat swollen, the skin is pink, the subcutaneous fatty tissue is well developed.
The skin of the newborn is covered with the so-called original cheese-like lubricant, the amount of which varies considerably. On the shoulders and back, the skin is covered with a soft down.
The chest of the newborn is convex, short, inactive. The limbs are short, the legs are slightly convex anteriorly and outwards, therefore they appear to be curved. The muscles are underdeveloped, especially the muscles of the limbs. For newborns, pronounced hypertension of the muscles is characteristic, especially of the flexor limbs. The movements of the upper and lower limbs are irregular. The voice is loud, persistent cry. Unconditioned reflexes (sucking, swallowing, sneezing, coughing, etc.) are quite well expressed. In boys, the testicles are descended into the scrotum, in girls, the small lips and clitoris are covered with large labia.
For a more accurate characterization of the condition of the newborn, the Apgar scale is currently used, making an assessment within the 1st minute after the birth of the child.
5. Apgar Scale
The test was proposed by anesthesiologist Virginia Apgar.
Virginia Apgar (English Virginia Apgar; June 7, 1909 - August 7, 1974) - American anesthetist in obstetrics. The author of the famous Apgar scale. Born June 7, 1909 in Westfield, New Jersey (USA) in the family of Helen Clark and Charles Emory Apgar. In 1929 she graduated from Mount Holyoke College, in 1933- Columbia University College of Physicians & Surgeons. In the same place in 1937 she graduated from the residency in surgery. After that, she studied anesthesiology and in 1938 returned to Columbia University as head of the anesthesiology department. In 1949, Apgar became the first female professor at Columbia P & S, while at the same time she was engaged in research and research work at Sloane Hospital for Women. In 1959, she received her Master of Public Health degree from Johns Hopkins University. In 1953, proposed a test for assessing the health of newborns, the so-called. Apgar scale.
The result, recorded a minute after birth and recorded again after 5 minutes, reflects the general condition of the newborn and is based on observations in five assessment categories. The condition of children who score from 7 to 10 points is considered good or excellent, and they usually need only ordinary care; those who scored from 4 to 6 points are in a satisfactory condition, and they may need only some resuscitation procedures; and those whose outcome is less than 4 require immediate assistance to save their lives. At one time it was believed that children, whose result after 5 minutes after birth remained low, are doomed in the future to have neurological problems, but recent studies have shown that most of these children grow up normal and completely healthy.
The assessment consists of the sum of the numerical indicators of five signs. With indicator 8-10, the condition of the newborn is assessed as good, with indicator 6-7 - satisfactory, and below 6 heavy. For example, in a newborn, the heart rate is 120 per minute (grade 2), irregular breathing movements (1), the limbs are somewhat bent (1), the reaction to a nasal catheter grimace (1), the skin color is pink, the limbs are bluish (one); The Apgar score is 6.
At an early age, the child begins the formation of complex brain functions, the rapid development of speech. Higher nervous activity improves, the limit of its working capacity increases (by the beginning of the second year the child can stay awake for 5 hours), conditional connections are easily and quickly formed, the second signaling system is formed, speech develops, sensorics are improved.
By the age of two, the child walks well, movements occupy a large place in his life. However, rapidly evolving mental processes, skills, and abilities are still in the formative stage, therefore they are not sufficiently stable. In addition, children of the second year of life are very easily excitable and difficult to adapt to any changes in living conditions. The resilience of the child’s body to various pathogenic influences is still sharply reduced, therefore at this age children are more susceptible, than children in their first year of life, to acute illnesses.
In the third year of a child's life, the intensity of physical development slows down, so characteristic of the first two years. The efficiency of the nervous system increases (the duration of wakefulness increases to 6-6.5 hours). There is a further development of speech, sensory, orienting-cognitive activity, improving movement. The course of development of a child of the third year of life depends on the level he achieved by two years. At the same time, as N.M. Aksarin, big changes in the psyche of children of the third year of life, as well as in mental development are associated with the development of speech. The vocabulary is rapidly increasing. Speech at this age becomes the main means of communication with adults and each other. The body’s resistance to the harmful effects of the environment and the physical endurance of the children gradually increase.
Describing the preschool period, N.М. Aksarina writes: “A child will be born without being able to pronounce a single articulate sound. In the first months of life, the articulation apparatus is improved by the child while he is walking, and from 7-8 months, hearing the sounds of a human voice, he begins to pronounce repeated syllables. of these lenative syllables forms the first 10-12 words. Then there is a period of some sort of lull - a slow growth of new words. During the first half of the 2nd year there is a rapid accumulation of understood words, the establishment of connections of the audible word and the ending Meta. The number of words that he actively uses increases slightly, by 1 year 5 months a child has only 30-40 words. In 1 year 5 months - 1 year 7 months there is a rapid jump (the rapid growth of new words), by 2 years the active dictionary is 300 - 400 words. At the 3rd year, the dictionary grows further (by 3 years - 1200-1300 words), the quality of speech is improved - pronunciation, construction, understanding. " The rapid pace of morphological and functional development of all organs and systems, the incompleteness of immunity contribute to the fact that young children fall ill from the most minor nutritional disorders and hygienic care. At the same time, each acute illness that has been transferred can lead to the development of chronic diseases, leading to a lag in the physical or psychological development of the child, between which there is a very large interdependence and unity.
With regard to early age, there are specific and specific development tasks that become the content of the work of both the psychologist and the teacher. Let us dwell on them in more detail.
First of all, this is the development of objective activity, since this activity at an early age is the leading one. It is in it that the child is introduced to the culture, the main psychological neoplasms of this period are formed in it: speech, visual-effective and figurative thinking, cognitive activity, purposefulness, etc. Within the framework of the subject activity, several directions can be distinguished, each of which is an independent task and implies certain implementation methods.
First, it is the development of culturally normalized, specific and instrumental actions. A small child must learn to use the surrounding objects “humanly”: eating a spoon correctly, drawing with a pencil, digging it with a handbag, combing a comb, fastening buttons, etc. This is not just a matter of developing hand movements and general motility. All these actions require overcoming spontaneous, impulsive activity, and therefore mastering oneself and one’s behavior. The child must understand and assign the meaning of these simple actions, see their result, feel their skill. All this gives him a sense of his competence, independence, self-confidence. To accomplish this task, from the age of 1, it is necessary to teach children to self-service: to show how to dress, comb, hold a spoon or a cup, leaving them the opportunity to act independently and encouraging them. In addition to the usual household procedures, we need special toys created for young children (knives, shovels, fishing rods with a magnet, etc.).
Another line of objective activity is the development of visual-effective thinking and cognitive activity. A young child thinks, above all, by acting with his hands. Correlating the shape or size of individual objects, he connects the properties of objects, learns to perceive their physical qualities. For such activities, there are numerous toys specifically designed for kids. These are all kinds of inserts of various shapes, pyramids, simple dolls, turrets, etc. By holding the balls through the maze or trying to open mysterious boxes, in which the coveted prize is hidden, the kid solves the most genuine mental tasks. And although the solution of these problems is inseparable from practical actions, it requires considerable mental effort and cognitive activity. The task of an adult here is not to show the correct course of action (that is, to suggest a solution to the problem), but to cause and maintain cognitive activity, to interest the child with a mysterious object and to induce independent experimentation.
Another major direction in the development of objective activity is the formation of the purposefulness and perseverance of the child’s actions. It is known that the activity of a child under 2 years of age has a procedural character: the kid enjoys the process of action itself, their result does not have any independent significance. By the age of three, the child already has a certain idea about the result of what he wants to do, and this idea begins to motivate the child’s actions. The child is no longer acting in such a way, but in order to obtain a certain result. Thus, the activity becomes targeted. It is obvious that focus on results, perseverance in achieving the goal is the most important characteristic not only of the child’s activities, but also of his personality as a whole. The help of an adult is necessary for the formation of this valuable quality. A small child needs to be helped to "hold" the goal, to direct him to achieve the desired result. For this you can use constructive games and toys that involve the receipt of a particular product. These can be figurative pyramids, from which you need to assemble a certain object (a machine, a soldier, a dog, etc.), all sorts of mosaics or puzzles that make up pictures, cubes or simple constructors for young children. All these games require a certain idea of what should happen, and perseverance in achieving the result.
All these types of substantive actions involve the individual work of the child. Small children still do not know how to act together; Objects and actions with them completely absorb the interests of children, they cannot be guided by the actions of a partner, take into account other people's desires, etc. Each child must have his own toy and his own ways of acting with it. Such individual activity with objects causes concentration and concentration on the subject, a kind of “fascination” with its actions. This is a very important and valuable condition. Montessori saw in the concentration of babies on actions with objects the beginning of the child's will. Therefore, it is necessary to fully support the individual work of the child with objects and create all possible conditions for it. This in turn requires a sufficient number of adequate benefits and special organization of the developing environment. Counseling teachers on the selection of the necessary toys, the creation of a game development environment, its periodic update - all these are the tasks of a psychologist who should be guided by the interests and abilities of children of a given age.
Another extremely important and responsible task of educating young children is the development of speech. Mastering speech, as you know, basically occurs precisely in this period - from a year to three. Speech rebuilds all mental processes of a child: perception, thinking, memory, feelings, desires. It opens up opportunities for completely new and specifically human forms of external and internal life - consciousness, imagination, planning, controlling one's behavior, logical and figurative thinking, and of course new forms of communication.
The speech of a small child arises and initially functions in communication with an adult. Therefore, the first task of education is the development of active, communicative speech. For this, it is necessary not only to constantly talk with the child, but also to include him in the dialogue, to create the need for his own statements. The child’s own speech does not develop through the imitation of strangers even by the most correct samples. In order for a child to speak, he must have a need for this, the need to express in words what cannot be expressed by other means. Such a speech problem (the task to say the right word) is set for an adult.
At the first stages of development, the baby’s speech is included in his practical substantive actions and is inseparable from them. A child can only talk about what he sees and what he does here and now. Therefore, the inclusion of words in concrete actions, (or "the unity of words and deeds") is a very important principle of forming active speech. Each new word should be clear to the child, carry a certain meaning and rely on a specific situation. The creation of such a speech-generating situation that activates the speech of children is a special psychological and pedagogical task, which should be solved in cooperation between a teacher and a psychologist.
Second important line speech development is the improvement of the so-called passive speech, i.e. understanding the speech of an adult. Most babies in 1.5-2 years already understand all the words and simple phrases when they are included in a specific situation. Overcoming situational connectedness and the formation of the grammatical structure of speech is the most important line of development at an early age. An invaluable role for this is the literature for kids. Short and simple children's fairy tales, rhymes by A. Barto or S. Marshak, folk songs and songs provide invaluable material for speech development. However, adults should open this material to kids, make it understandable and attractive. To do this, you need expressive reading, which is accompanied by gestures, bright intonations and possibly a play of toys. The development of methods of speech development of young children is also included in the tasks of a psychologist.
At an early age, another important function of speech arises - regulatory. Appears the ability to control their behavior with the help of the word. If up to 2 years of age, the child’s actions are determined mainly by the perceived situation, then in the second half of early age it is possible to regulate the child’s behavior through speech, i.e. performance of speech instructions of the adult. Psychologists regard this form of behavior as the first stage in the development of arbitrary behavior, when the child’s actions are mediated by a speech sign, which is directed towards their behavior. Therefore, the action according to the instructions opens up the possibility of developing self-regulation and self-control. This essential ability should be developed and exercised. It is important to choose for each child a certain level of complexity of the instruction, which corresponds to its capabilities and abilities. This is a very significant line in the development of a child at an early age, which needs appropriate psychological and pedagogical support.
Mastering speech at an early age makes the development of children's imagination possible. Imagination arises in the third year of life, when the ability to play substitutions appears, when familiar objects are endowed with new names and begin to be used in a new capacity. Such game replacements are the first form of imagination of the child and constitute the most important step towards the new leading activity of the child - the role-playing plot game. Numerous observations and studies show that the game does not arise by itself, without the participation of those who already know how to play - adults or older children. A small child needs to be taught to play. Learning the game is of course not in the classroom, but in the process of playing together with an adult who gives the child a way to replace some items with others. Playing kids requires the indispensable participation of an adult who not only gives them the necessary ways of playing actions, but also "infects" them with interest in activities, stimulates and supports their activity. Any game has a complex educational impact: it requires both mental, and volitional, and physical effort, and coordination of its actions, and of course (if the child is truly included in it) brings emotional satisfaction. Therefore, the development of creative games and imagination in children 2-3 years is the most important task of the psychologist.
At an early age, another extremely important area of the child’s life activity arises - his communication and relationships with peers. Despite the fact that the need for a peer is far from the main place at an early age and is usually not considered as the main line of its development, the first forms of interaction between children play an extremely important role for the development of the child's personality and the further development of interpersonal relations. This is where the feeling of immediate community and connection with other people, equal to a child, is laid. Studies show that the need to communicate with peers arises in the third year of life. At this age, communication between children has a very specific content, which is an emotional-practical interaction. A special place in this interaction takes imitation of each other. Children, as it were, infect each other with common movements and emotions and through this feel mutual commonality. Such an interaction gives the child a sense of its resemblance to another being equal to it. The experience of similarity and community causes great joy and promotes self-awareness. The educator can give it a cultural, organized form. The best means for this is the well-known games in which children act simultaneously and equally - Karavai, Carousel, Inflate the bubble, Bunny, etc. These games at an early age should take place with the direct participation of an adult who organizes children, shows them the necessary movements and words, immerses them in the overall atmosphere of the game. Development, selection and conduct of such games is an important area of work of the psychologist.
Almost all young children (from 1.5 years old) growing up in a family need contacts with peers and master communication skills. At the same time, early childhood is a sensitive period for the formation of a tolerant attitude towards others. Therefore, it is very expedient to unite children with various difficulties in one group. Such an association of different children at an early age is very effective. For children with special needs, this makes it easier for their peers to adapt to society and speeds up their development, while ordinary children will be given an irreplaceable experience of communicating with other, different people, which is extremely important for nurturing tolerance. At the same time, the correct organization of communication among the children in the integrative group presents serious difficulties and requires the participation of professional psychologists.
All of these tasks are common to the teacher and psychologist and are solved in their close cooperation.
Thus, the development of young children is the most amenable to pedagogical influences period. Everything is mastered and known for the first time. There are no skills, no ideas, knowledge. But the predisposition to assimilation is great, learnability is high, since there are innate mechanisms that serve as the basis for the formation of mental qualities peculiar only to man. But this is also the most vulnerable period in a person’s life, requiring the greatest care from adults.
It was at this time that the experience of interacting with parents, other family members, children and adults influences the development of the child.
The needs of young children in health, nutrition, a safe environment, psychosocial and cognitive development must be met in a coordinated and interconnected way so that each of the components supports the other and none is left unattended.
It is extremely important for the development of moral concepts the formation of the emotional experience of a young child. All information must be permeated with feelings. The concepts of good and evil, happiness and sorrow, and even the concept of a bright morning, a hot summer, a dangerous trip, a cozy room and an old couch are formed only when the child directly observes the manifestations of feelings and emotions that characterize these concepts.
For the development and upbringing of young children, it is necessary to comprehensively support the child’s individual development, which promotes favorable adaptation and the formation of initial social experience based on the satisfaction of vital needs.
The main objectives of the development of young children include:
protection and promotion of psychophysical health, the formation of competencies necessary for life;
the creation of favorable conditions for the flow of the sensitive period of the child's sensorimotor and speech development;
fostering a positive attitude and a basic sense of trust in people (the primary foundations of morality), cultivating the positive moral feelings of children;
emotional development;
activization of work with the family for the purpose of psycho-pedagogical education of parents for the care of young children, their upbringing and development.
For the successful development of young children, certain pedagogical conditions are needed, which will be discussed in the next paragraph.
- Riddles for girls on 8
- When on the ship two flags
- Order on the creation of the duty dispatch service
- Historical flags of the states of 1700
- The role-playing game as the main type of games for preschoolers place in the structure of children's games
- Logic Tricks for Adults
- Medical Institute with budget places